WIC’s Critical Benefits Reach Only Half of Those Eligible
States Missing Out on Opportunity to Improve Pregnancy-Related, Child Health
The federally funded WIC program — the Special Supplemental Nutrition Program for Women, Infants, and Children — improves lifetime health for low-income pregnant and postpartum people, their infants, and young children, but just half of those eligible are enrolled. This underutilization has no single cause and has occurred despite adequate funding to serve all eligible applicants for more than 25 years. While there is some uncertainty about whether the bipartisan commitment to providing enough funding to serve all eligible families who seek WIC services will be maintained in the future,[2] if it is, governors and state policy officials, program administrators, health care providers, and the maternal and child health community can all take steps to help more eligible families enroll in this vital program.
WIC is a cost-effective program that provides nutritious foods, nutrition education, breastfeeding support, and referrals to health care and social services to over 6 million people in low-income families.[3] It has been part of the nation’s nutrition safety net for over 45 years. Extensive research shows that participating in WIC leads to healthier infants, more nutritious diets and better health care for children, and later to higher academic achievement for students.[4]
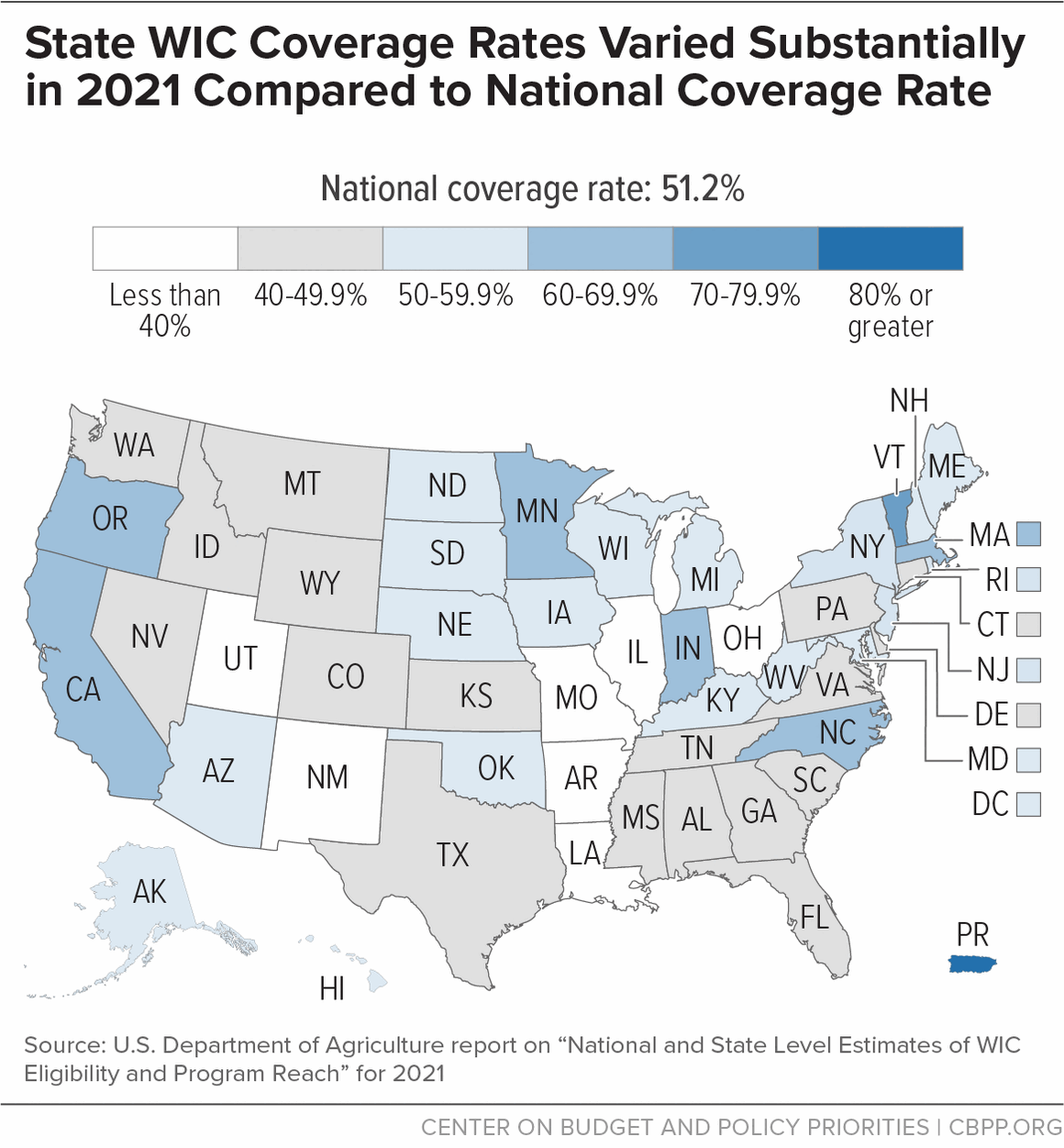
Yet only 51.2 percent of eligible individuals participated in WIC in 2021, well below earlier years, according to the most recent U.S. Department of Agriculture (USDA) annual estimates.[5] Coverage rates vary widely by geography and participant group.
- Across states, coverage rates range from 34.6 to 71.6 percent.
- Some 78.0 percent of eligible infants participated, but just 43.2 percent among children aged 1 through 4 did.
- Eligible postpartum people participated at higher rates (67.2 percent) than eligible pregnant people (43.7 percent).[6]
- People living in metropolitan areas participated at more than twice the rate (56 percent) of those living in non-metropolitan areas (23 percent).
- Hispanic people (58.1 percent) and Black people (48.5 percent) had higher coverage rates than white people (44.2 percent).[7]
- More than half of WIC-eligible people receiving Medicaid or SNAP did not access WIC, with more than 4 in 5 WIC-eligible pregnant Medicaid enrollees missing out.
WIC participation is associated with reduced risk of premature birth, low birthweight, and infant mortality. This is especially important because pregnancy-related complications and mortality, as well as infant mortality, are higher for families of color than for white families due to unequal access to health care and broader inequities in health, economic, and other systems for people of color.
Thus, increasing WIC coverage across the board — and for pregnant people of color and their infants in particular — can be an important part of a strategy to improve pregnancy-related and child health, mitigate the large pregnancy-related health disparities affecting these communities, and advance racial equity in other aspects of pregnancy-related and child health and food security.
WIC utilization can be measured in two ways. WIC coverage rates show the share of eligible people who participated in the program during a calendar year. USDA estimates coverage rates for each year retrospectively by comparing the number of WIC participants to the estimated number of people who were eligible. The most recent USDA coverage rate estimates are for 2021. WIC participation data show the number of people participating in the program. USDA publishes participation data each month for each state agency, and data for past years remain available.[8]
While WIC coverage rates for 2022 and 2023 are not yet available, nationwide participation increased by 5.3 percent between fiscal year 2021 and fiscal year 2023, rising most rapidly during 2023. This trend is a promising sign that participation among eligible families may be regaining some lost ground.
Most states experienced participation growth over this period, but state changes in WIC participation ranged from a 20 percent decrease to a 22 percent increase. In 22 states, participation grew at more than the nationwide rate; in 17 states, participation grew but at less than the nationwide rate; and in 11 states, the District of Columbia, and Puerto Rico, participation fell.[9]
State variation in participation trends suggests that state policies and practices can affect WIC utilization. To reverse participation declines, some state and local WIC program administrators are streamlining WIC enrollment practices, partnering with other programs to reach WIC-eligible individuals, and employing other strategies to recruit and retain participants. For example, some states have begun communicating with participants using social media, text messaging, and WIC apps and have adopted electronic approaches for viewing or receiving eligibility documentation and information for nutrition assessments. Many states have set up online pre-application and appointment request forms.
Even before the pandemic, some states increased telephone and videoconferencing options for nutrition education and other appointments, and those options are now more widely available. But remote appointments and other innovations are by no means universal. Options for remote appointments may be especially important for families living in non-metropolitan areas, where families with children under 5 are more likely to be food insecure.
The 2021 American Rescue Plan’s $390 million investment in WIC outreach, modernization, and innovation is helping state and local agencies replicate promising practices and explore new approaches, an important step toward increasing WIC utilization. By exploring and adopting more such practices, policymakers and program administrators can get WIC’s valuable benefits to an even larger share of those eligible over time.
This report explains why increasing WIC take-up matters, summarizes WIC coverage rates over time and among specific groups, identifies likely participation barriers, and highlights specific strategies that state and local WIC leaders can employ to reduce barriers so more eligible families will enroll and participate for longer. The Appendix provides resources to help WIC administrators pursue these strategies. We’ve also published state-by-state fact sheets showing WIC coverage rates and participation over time across various categories, along with maternal and child health measures and an estimate of the additional funding each state would have received with a higher coverage rate.[10]
Increasing WIC Utilization Can Have Widespread Benefits
The benefits of increasing WIC participation extend beyond individuals and their families to communities and states. WIC improves perinatal outcomes, reduces food hardship, and reduces racial and ethnic health disparities; it provides billions of dollars annually to support food production and sales in grocery stores and farmers markets; and studies show that it generates Medicaid savings by improving pregnancy-related and child health. With 100 percent federal funding (WIC does not require states to provide matching funds or cover program administration), WIC is available in all states and in communities of all sizes.
Improving Pregnancy-Related and Child Health
Pregnancy-related complications and deaths, among both parents and infants, are alarmingly high, especially among Black and Hispanic people. Babies fare worse in the U.S. than in almost all other developed countries, and the maternal mortality rate in the U.S. is more than double the average for developed countries.[11] Black and Hispanic people are at significantly higher risk for severe pregnancy-related health complications such as preeclampsia, due in part to lack of access to care.[12] Pregnancy-related deaths are much rarer than other serious pregnancy-related health issues but have increased substantially over the past three decades, even though most are preventable.[13]
Moreover, racial and ethnic disparities in pregnancy-related mortality are striking and persistent.[14] Black people are three times likelier to die due to pregnancy than white people. Black people over age 30 and Black people with at least a college degree are four or five times likelier to die due to pregnancy than their white counterparts. Infants who are Black are also at higher risk, as are those who are American Indian, Alaska Native, Native Hawaiian, and other Pacific Islander. They have higher shares of preterm births, low-birthweight births, or births for which they received late or no prenatal care compared to white infants, and they are roughly twice as likely to die as infants of white people.[15]
Health coverage during pregnancy and the postpartum period is particularly important in addressing life-threatening conditions.[16] Extensive research over four decades shows that participating in WIC improves nutrition and health, including infant health and mortality:[17]
- WIC participants give birth to healthier babies who are more likely to survive infancy than those born to eligible non-participants. Study after study links WIC participation during pregnancy with longer gestations, higher birthweights, and generally healthier infants, and the effects tend to be greatest for children born to the most disadvantaged mothers.
- Children in low-income families who participate in WIC are as likely to be immunized as more affluent children and more likely to receive preventive medical care than children in low-income families who don’t participate.
- Children whose mothers participated in WIC while pregnant scored higher on assessments of mental development at age 2 than similar children whose mothers did not participate, and they later performed better on reading assessments while in school.
- Children who consistently participate in WIC up to age 5 have better overall diet quality, on average, than children who only participated at ages 1 and 2.
Thus, increasing WIC coverage can play a crucial role in improving pregnancy-related and child health outcomes and mitigating related racial and ethnic disparities. Recognizing this, Congress directed USDA to assess WIC’s impact on reducing maternal mortality among populations with the highest rates, using existing evidence as well as evidence gathered in the future to monitor progress over time.[18]
Reducing Food Insecurity
WIC can play an important role in reducing food insecurity and mitigating racial and ethnic disparities in food hardship. In 2022, 12.8 percent of U.S. households experienced food insecurity, meaning they could not afford enough food at some point during the year, up from about 10.2 percent in 2021. Households with children under age 6 were likelier to face food insecurity; 16.7 percent were food insecure, up from 12.9 percent in 2021. And in roughly half of those households, the children themselves were food insecure.[19]
There are also racial disparities in food insecurity rates due to long-standing barriers to housing, education, and employment opportunities for people of color. Households with children under 18 who are Black or Hispanic were more than twice as likely to be food insecure (27.9 percent and 24.7 percent, respectively) than white households (12.3 percent) in 2022. Households of another race or multiple races had a food insecurity rate of 12.4 percent.[20] In 2022, among households with children under 5, the children themselves were more likely to be food insecure in Black (15.1 percent) and Hispanic (13.0 percent) households than in white households (5.3 percent). Children themselves were food insecure in 5.5 percent of households of another race or multiple races.[21]
Food insecurity raises serious concerns about the long-term consequences for children’s health and development — particularly for children of color, given their much higher food insecurity rates. Studies link food insecurity among children with reduced intake of some key nutrients, health problems such as iron deficiency (which is linked with long-term neurological damage), and behavioral issues and mental health conditions. These problems can, in turn, lower children’s test scores, their likelihood of graduating from high school, and their earnings in adulthood. Even short periods of food insecurity pose long-term risks for children.[22]
Longer periods of WIC participation for pregnant people and children are associated with less food insecurity and improved nutritional outcomes for children. Also, children who participate in both WIC and the Supplemental Nutrition Assistance Program (SNAP) are likelier to be food secure later in life than children who only participate in SNAP.[23] While WIC take-up is higher for lower-income families,[24] who are at greater risk of food insecurity, improving WIC coverage rates could lower food insecurity in households with young children and reduce racial disparities in food insecurity.
Helping State Budgets and Economies
In addition to improving pregnancy-related outcomes, enhancing child health, and reducing food hardship, increasing participation in WIC can benefit state budgets and economies. By improving pregnancy outcomes and child health, WIC may lower Medicaid costs. A 1992 study found that for every $1 spent on WIC during pregnancy, the Medicaid savings during the first 60 days of life ranged from $1.77 to $3.13.[25] A more recent study found that the improved birth outcomes for each additional $1 in spending on prenatal WIC services result in Medicaid savings ranging from $1.24 to $6.83.[26]
Also, when WIC utilization increases, more families can purchase nutritious food in local grocery stores. For each percentage point rise in WIC coverage in 2021, about 121,000 more people nationwide would have benefited, nearly $40 million more in federal funding would have been available to provide nutrition services, and over $80 million more would have been available to purchase food and support local food systems. In 2023, WIC benefits allowed shoppers to purchase more than $4 billion in food, supporting jobs in retail grocery stores as well as in agriculture, food processing, and distribution.[27] In many states, WIC participants can also purchase fruits and vegetables at farmers markets, directly benefiting local farmers.
Share of Eligible People Who Receive WIC Has Fallen, But Participation Is Increasing
Only about half (51.2 percent) of those eligible for WIC participated in the program in 2021 according to USDA, which administers WIC.[28] The WIC coverage rate — the share of eligible individuals who participate — remained steady between 2019 and 2020, a testament to the program’s resilience as the pandemic set in, parents lost work, and its operations had to transform overnight. It declined slightly in 2021, continuing a downward trend since 2016.
The WIC coverage rates for 2016-2020 are not comparable to earlier data due to a change in USDA’s methodology for estimating the eligible population. Nonetheless, we can compare earlier trends to more recent ones. USDA data from an earlier report show WIC coverage declined from a peak of 63.5 percent in 2011 to 52.7 percent in 2015.[29] Similarly, USDA data show a gradual decline from 54.2 percent in 2016 to 51.2 percent in 2021 in the most recent report, suggesting troubling downward trends over the last decade. (See Figure 1.)

Although estimates of coverage rates more recent than 2021 are not yet available, participation has increased since then. Between fiscal year 2021 and fiscal year 2023, average monthly participation grew by 5.3 percent nationwide, increasing the average number of people served each month by 330,000.
The participation increase does not necessarily mean that coverage has increased because estimates of the number of eligible people over this period are not yet available. But the increase is a promising sign that the share of eligible people who participate may be increasing and a sure sign that WIC is providing assistance to and improving the health outlook for more families.
Coverage Decline Affects All Races and Ethnicities
Hispanic families (58.1 percent) and Black families (48.5 percent) had higher coverage rates than white families (44.2 percent) in 2021. But the share of eligible Hispanic and Black people receiving WIC fell by 8.1 and 7.1 percentage points, respectively, between 2016 and 2021. For white people, the coverage rate ranged from 41.6 percent to 45.4 percent over that period. In a promising development, coverage increased by 6.6 percentage points for people of another race or multiple races. (See Figure 2.) We are unable to assess more recent trends because participation data do not include race or ethnicity.

As explained above, people of color are much likelier than white people to experience adverse pregnancy-related and infant health outcomes such as pregnancy complications and maternal and infant mortality. They are also likelier to experience food insecurity. So it is noteworthy that despite declines in coverage rates over the 2016-2021 period, Hispanic people had the highest WIC coverage rate in 2021 (58.1 percent), followed by people of another race or multiple races (55.7 percent), Black people (48.5 percent), and finally white people (44.2 percent). Given the strong evidence that WIC supports healthier pregnancies and births, the program may already be reducing racial disparities in health and food insecurity.
Yet even with their higher coverage rates, more than one-third of eligible Hispanic people missed out on WIC in 2021, as did half of eligible Black individuals. Increasing WIC coverage rates across racial and ethnic groups could alleviate the nationwide crisis in pregnancy-related health issues while also contributing to gains in racial equity in pregnancy-related outcomes, child health, and food security. Our state fact sheets include estimated state coverage rates by race to help state leaders and stakeholders target outreach and retention efforts.
WIC Utilization Varies Widely by State
WIC coverage rates vary considerably from state to state, from 34.6 percent to 71.6 percent in 2021, suggesting that state administration of the program can significantly affect access to WIC.[30] In 2021, seven states saw fewer than 40 percent of eligible people participate; only in two states and Puerto Rico did more than 65 percent of eligible people participate. (See Figure 3.)
Although coverage estimates more recent than 2021 are not yet available, participation data show sizable variation in changes since 2021 among states.[31] Between fiscal year 2021 and fiscal year 2023, participation grew by 5.3 percent nationwide. While most states experienced participation growth over this period, state changes in WIC participation ranged from a 20 percent decrease to a 22 percent increase. In 22 states, participation grew at more than the nationwide rate; in 17 states, participation grew but at less than the nationwide rate; and in 11 states, the District of Columbia, and Puerto Rico, participation fell.[32] Monthly participation data since fiscal year 2021 are included for each state in the state fact sheets.
WIC Utilization Lowest for Pregnant People, 1- to 4-Year-Olds
Coverage rates in 2021 were lowest among pregnant people and non-infant children, as they have been each year since 2005. While take-up by new and expecting parents are both alarmingly low, only 43.7 percent of eligible pregnant people participated, compared to 67.2 percent of eligible postpartum people. As a result, over 600,000 WIC-eligible people went unserved in 2021 during some or all of their pregnancy, missing out on the nutrition services and food assistance that have been shown to improve pregnancy outcomes.
Over 4 million eligible 1- to 4-year-olds — more than a quarter of all children of that age — also missed out on WIC’s health and developmental benefits. While 78.0 percent of eligible infants participated, only 64.3 percent of eligible 1-year-olds and 24.7 percent of eligible 4-year-olds did. (See Figure 4.) And while coverage rates vary by state, in every state the rates are lower for adults and children than for infants (USDA does not develop separate state-level estimated rates for pregnant versus postpartum people).

While WIC coverage rates for 2022 and 2023 are not yet available, participation data show that the monthly average number of children aged 1 to 4 served during fiscal year 2023 was 6.4 percent higher than in fiscal year 2021. This could be a promising start to reversing the downward trend in child participation, but filling the sizable coverage gap will require an ongoing commitment to addressing the barriers to participating in WIC. Another promising development: after falling in fiscal year 2021, the average number of pregnant people served each month increased by 2.1 percent in fiscal year 2022 and by 5.7 percent in fiscal year 2023.[33]
Many SNAP, Medicaid Participants Not Participating in WIC
Pregnant and postpartum people, infants, and children under age 5 who receive Medicaid or SNAP benefits are automatically considered income-eligible for WIC, but many do not participate. Eligible families’ take-up of Medicaid and SNAP is much more robust than it is for WIC.[34]
USDA estimates that nationwide, more than half of WIC-eligible people receiving Medicaid or SNAP (or both) did not access WIC in 2021, and much higher shares of certain groups missed out on WIC.[35] Among WIC-eligible Medicaid enrollees with incomes at or below 185 percent of the federal poverty guidelines (WIC’s limit for families not enrolled in these programs), only 16.9 percent of eligible pregnant people and 41.1 percent of children aged 1 through 4 participated in WIC. (See Figure 5.) Similar percentages of pregnant people (12.9 percent) and children (42.6 percent) enrolled in SNAP but not Medicaid participated out of all who were eligible for WIC. (See Figure 5.)

By not only measuring the overall gap but analyzing the gap based on specific criteria — such as geography, WIC category (pregnant, postpartum, infant, or child aged 1 through 4), or race — states can design targeted enrollment and retention strategies. State WIC agencies can work with state Medicaid agencies to automatically refer Medicaid applicants and enrollees to WIC and to promote referrals by managed care organizations, health care providers, and community-based health workers.[36]
For example, in some states the WIC agency is partnering with the Medicaid and/or SNAP agency to identify enrollees in those programs who are eligible for WIC but not participating.[37] This strategy is working; states have demonstrated that targeted outreach and streamlined enrollment for families who are income-eligible for WIC but not enrolled can improve WIC certification rates.[38]
How to Increase WIC Utilization
While the recent increase in WIC participation is promising, more work is needed to enroll additional eligible families and reverse the decline in coverage rates. State officials and program administrators can enhance their efforts by assessing the barriers families experience in accessing and participating in WIC and by identifying opportunities to encourage families to take part in the program for as long as they are eligible.
WIC’s coverage rate decline through 2021 is not due to lack of funding. Since 1997, policymakers have provided enough WIC funding each year to serve all eligible families who seek to participate; eligible families have not been turned away or placed on waiting lists. While currently there is some uncertainty about whether enough funding to serve all eligible families who seek WIC services will be provided for fiscal year 2024, that uncertainty does not affect the coverage rates or participation data discussed in this report.[39]
WIC’s ability to serve all eligible participants partly reflects the program’s cost-effectiveness. WIC employs a highly effective competitive bidding system that obtains infant formula at a substantial discount. While food prices rose by 29 percent between fiscal years 2009 (when the current WIC food benefit packages were implemented) and 2022, the cost of WIC foods rose by just 13 percent, even with a substantial increase in fruit and vegetable benefits starting in 2021.[40]
Nor are eligibility restrictions a factor. Congress and USDA periodically change WIC operations and benefits through program reauthorizations and revisions to federal regulations, such as updates to WIC food packages. While these changes may affect WIC processes and benefits, there have been no changes to eligibility requirements that would reduce the number of people eligible to take part in the program.
To some extent, the downward trend in WIC utilization reflects the program’s historical success. As an effective program that has widespread bipartisan support and is fully federally funded, WIC operates “outside the spotlight.” Because state officials have not had to respond to concerns about the program, they could focus on other aspects of the health care and food assistance landscape. But that lack of attention has resulted in missed opportunities for coordination between WIC and other programs for outreach, joint applications, and integrated services that might help WIC reach more eligible families. Similarly, in many states, WIC has not been consistently represented in cross-agency efforts to improve pregnancy-related outcomes and child health.
Until Congress began providing sufficient WIC funding to serve all eligible applicants in 1997, funding was the limiting factor on participation. Then, however, the number of WIC participants rose every year between fiscal years 2000 and 2010. Thus, program administrators were not accustomed to having to promote the benefits of WIC to increase enrollment or revamp its service delivery to attract eligible families. While the COVID-19 pandemic accelerated modernization in some areas, such as remote appointments and electronic submission of documents, modernization still lags in others — for example, online appointment scheduling and online shopping are rarely available — affecting applicants’ and participants’ experiences with the program and thus their decisions about whether to continue participating. [41]
The rest of this section describes factors that contribute to underutilization of WIC and strategies to help address them. The Appendix shares suggestions for implementing the strategies along with resources. Many of the resources included in the Appendix contain examples of policies and practices WIC state agencies are currently using.
Misinformation and lack of information. Some families incorrectly believe they are not eligible for WIC. Some common misconceptions are that WIC is not available to families with a working adult, is only available to infants up to 1 year old or to people enrolled in Medicaid, or only provides infant formula. Sometimes relatives do not realize that they can apply for WIC benefits for the children in their care.
In addition, families that include immigrants may have concerns that receiving WIC benefits could affect their ability to change their immigration status or to have a family member come to the U.S. While receipt of WIC does not affect such immigration issues, there is significant fear and misinformation among immigrants.
Health care providers, child care providers, and community-based organizations serving WIC-eligible individuals may lack information about the program and how to refer families. Making accurate information widely available through outreach to eligible families and partnerships with health care providers and organizations that serve low-income families is an ongoing responsibility of state and local WIC programs.
Difficulty accessing services. For decades, WIC appointments occurred almost exclusively as in-person visits at WIC clinics that were not affiliated with other government services and often lacked convenient locations or business hours. Parents were required to bring their children to enrollment appointments and to provide paper copies of eligibility documents. Appointments could take well over an hour for eligibility determination, nutrition assessment, and counseling before a family could begin receiving food benefits. Most follow-up visits for nutrition education or mid-certification assessments were also conducted in person.
Fortunately, state and local agencies now have a number of options to schedule appointments in more convenient places and at more convenient times, as well as to make the appointments themselves more productive. For example, under state waivers provided by USDA during the pandemic and extended through the American Rescue Plan, WIC applicants and participants have the option for telephone or videoconference appointments for enrollment and periodic recertification. (Even before the pandemic, some states had begun offering online and remote nutrition education and breastfeeding services.) This flexibility reduces the time and effort associated with in-person visits to WIC clinics and, as noted in the text box above, may be especially important for families living in non-metropolitan areas with limited or no access to public transportation.
WIC families need appointment options that accommodate work, school, and transportation schedules and the flexibility to easily reschedule if needed. By offering appointments during lunch hours, early evening, and/or Saturdays and by setting up portals or mobile apps that enable participants to view and change their appointments, agencies may improve appointment attendance and program retention.
State agencies can also shorten and simplify certification appointments by adopting practices such as offering online applications or pre-applications, permitting families to send or share eligibility documents electronically, obtaining measurements from health care providers, and streamlining the nutrition assessment. The variation among states offers an opportunity to identify practices that streamline the eligibility process and make certification appointments easier for both participants and staff.[42]
Federal WIC regulations and USDA guidance, including new guidance on streamlining WIC certification documentation,[43] give state agencies flexibility to further streamline and modernize policies and processes they use to determine and document eligibility. USDA also provides several training tools to support state and local agencies in providing individualized, high-quality nutrition assessment, nutrition education, and breastfeeding services. Applying best practices in nutrition services makes WIC appointments more valuable to participants.
Participants have responded very favorably to the changes states have already made. In a survey of nearly 23,000 participants across 12 states, 75 percent rated the quality of phone, video, online, and curbside WIC appointments during COVID as equal to or better than in-person appointments before the pandemic. Most survey respondents reported that remote interactions not only reduced COVID risks but also were easier (because they didn’t require taking children to WIC sites), saved time and money (because they didn’t involve travel), and didn’t cause participants to miss work or school.[44] These practices are important to build on in the coming years.
Lack of state coordination across programs. Many prenatal and postpartum individuals and families with young children do not know they may be income-eligible for WIC if they receive Medicaid, SNAP benefits, or Temporary Assistance for Needy Families (TANF, which replaced Aid to Families with Dependent Children) or have certain family members eligible for Medicaid or TANF. Program administrators and personnel of those programs may also be unaware of this or may be unsure of how to make WIC referrals. State government structures can create barriers to collaboration between WIC and these other programs when they are administered by different departments or agencies.
By overcoming organizational barriers to coordination between WIC, Medicaid, and SNAP, states can facilitate ongoing training, data sharing, targeted outreach, and improved referral processes, which are important ways to strengthen WIC participation.
Challenges with shopping. Federal rules prescribe the types and quantities of WIC foods available to participants, but state WIC agencies determine which brands, package sizes, and (for some foods) forms can be purchased.[45] States also choose which of the available food package substitutions for cultural or family preferences to allow and how to offer these flexibilities to participants. These decisions affect participants’ perception of the value of WIC foods for their family; they can also influence how easy or difficult it is to shop for WIC foods.
The shopping experience is also affected by state decisions about where WIC benefits can be used and the type of electronic benefit transfer (EBT) system selected. WIC state agencies are required to enter into agreements with retail grocery stores to authorize them as “vendors” to redeem benefits for WIC shoppers, and they are required to monitor stores for compliance with federal and state rules. State decisions about the types and locations of vendors to authorize affect participants’ access to stores where they can shop for WIC foods.
Similarly, while all states are required to provide participants with electronic cards to shop for WIC foods, they can choose either online or offline cards. While participants have responded favorably to cards of both types, offline cards require more in-person visits to WIC because food benefits cannot be loaded on them remotely. The result is that participants must take their EBT card to a WIC clinic at least once every three months for benefits to be loaded, with additional trips to the clinic if benefits need to be changed. The advantages of providing participants with remote appointments are undermined when a remote appointment results in a benefit change that necessitates a trip to the WIC clinic.
Some states now offer options to make shopping easier, such as apps to help locate stores that accept WIC or to identify eligible foods, self-checkout lanes, and curbside pick-up. Several states are participating in an online shopping project funded by USDA.[46] Practices that make it easier for participants to use their WIC food benefits without stigma or hassle are important for encouraging full use of benefits and ongoing participation.
State policies and priorities. While WIC programs operate under a set of federal rules and policies, state WIC agencies have considerable flexibility to determine practices that affect how burdensome it is to enroll, receive services, and shop using WIC benefits. In addition to the areas described above, state agencies are responsible for allocating WIC grant funds for local services, maintaining WIC information systems and technology, tracking benefit issuance and paying for redeemed food benefits, monitoring retail grocery stores, and other operational decisions.
State-level priorities and decisions affect the WIC experience for both applicants and participants. Ongoing reviews and refreshes of state policies, practices, and systems are essential to ensure they minimize burden, incorporate available flexibilities and technology, and promote participant-centered services.
Federal Funding Available to Support State Improvements
As explained above, a number of state WIC agencies have been updating systems, policies, and practices to make it easier for eligible families to access and use WIC services. Federal policymakers have supported state efforts by making funding available for technology upgrades and pilot projects to test new approaches for serving participants. They quickly approved waivers that made it possible to offer appointments and issue benefits remotely, along with other flexibilities that state agencies requested at the beginning of the pandemic and extended them throughout the public health emergency. The Rescue Plan provided waiver authority that will allow remote appointments to continue through September 2026.[47]
With funding available through the Rescue Plan, USDA has awarded grants to state agencies for WIC outreach, modernization, and innovation. Rescue Plan funds are also being invested in projects to pilot WIC online shopping, conduct community innovation and outreach, and assist state agencies with data matching and targeted outreach to WIC-eligible enrollees in Medicaid and SNAP.
During 2022, USDA awarded grants of $350,000 each to state WIC agencies for projects to develop a modern WIC experience at the state and local level by introducing technology that works for both participants and staff, improving communication (including to people with limited English proficiency), and incorporating human-centered design and user feedback in decisions about program changes.[48] In 2023, all state agencies received grants ranging from $750,000 to over $5 million for projects to modernize WIC by improving communication and reducing participant/applicant burden associated with interacting with WIC, streamlining local operations related to the participant experience, establishing measures and mechanisms for collecting participant feedback and ongoing program evaluation, and improving the shopping experience.[49] State agencies can use these funds through September 2027.
Funding will also soon be available to state WIC agencies to use Medicaid and SNAP data to identify families who are eligible for WIC but not enrolled, conduct targeted outreach to them, and measure the effectiveness of this strategy to increase WIC take-up.[50] These funding streams provide a unique opportunity for states to address barriers and implement strategies to increase WIC participation.
Take Action to Increase WIC Participation
WIC is a vital nutrition and food assistance resource that is underutilized in all states. By implementing strategies to increase WIC participation, states can improve pregnancy-related and child health, reduce food hardship among families with children, and strengthen state and local food systems. WIC is federally funded and states have received additional multi-year federal grants to support modernization, so state funding is not needed to make these program improvements. By leveraging promising practices initiated during the pandemic along with new federal policy flexibilities, states have a unique opportunity to build on recent increases in participation to reach a greater share of eligible families and improve their health and well-being.
Appendix
See the WIC Hub at https://thewichub.org/, hosted by the National WIC Association, for additional resources, including examples from state and local WIC programs.
| Resources | ||
|---|---|---|
| Enhance Outreach and Referrals | ||
| Strategy | Implementation | Resources & Examples from Other States |
| Send targeted outreach messages to eligible families. | Work with partners to:
| View the toolkits “Increasing WIC Coverage Through Cross-Program Data Matching and Targeted Outreach” at https://www.cbpp.org/wicdatamatchingtoolkit and “Assessing Your WIC Certification Practices: Targeting Outreach” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-targeting See how state agencies are coordinating with Medicaid and SNAP to reach WIC-eligibles at https://www.cbpp.org/wiccollaborationsurvey Review the FNS policy, “Data Sharing to Improve Outreach and Streamline Certification in WIC,” at https://www.fns.usda.gov/wic/data-sharing |
| Continuously educate health care and child care providers, as well as community-based social service organizations, about WIC eligibility and services. | Routinely communicates with partners to:
| View the toolkit “Assessing Your WIC Certification Practices: Coordinating Services” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-coordinating See “WIC Guide for Health Care Providers” at https://frac.org/research/resource-library/wicguidehealthcareproviders and “New Jersey WIC Toolkit: Helping Pediatric Practices Help Families” at https://www.nj.gov/health/fhs/wic/documents/toolkit/WIC_FI_Toolkit.pdf |
| Develop and promote referral mechanisms for health care providers, child care providers, and community-based social services organizations. | Work with partners to:
| View the toolkit “Assessing Your WIC Certification Practices: Facilitating Enrollment” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-enrollment Review “2023 WIC Technology Landscape Report” at https://media.nwica.org/2023%20wic%20tech%20report%204.5.23.pdf See an example of health care provider referral forms for Massachusetts WIC at https://www.mass.gov/info-details/wic-medical-referral-forms See an example of referral reports included in the Colorado WIC Data Dashboard at https://www.coloradowic.gov/partners-quarterly-report-dashboard |
| Partner with community-based organizations to conduct outreach. | Join with partners to:
| Through a cooperative agreement between USDA and the Food Research & Action Center, federal funding is available to support innovative outreach efforts to increase participation and equity. 36 projects were funded in May 2023, and another funding opportunity is forthcoming. See “WIC Community Innovation and Outreach Project” at https://frac.org/wic-ciao andhttps://www.hellowic.org/projects/ Review “Enhancing Participant-Centered Services Between the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) and Head Start Programs” at https://wicworks.fns.usda.gov/sites/default/files/media/document/10_Ways_WIC_and_Head_Start_Can_Collaborate.pdf |
| Improve Access, Convenience, and Quality of WIC Services | ||
|---|---|---|
| Strategy | Implementation | Resources & Examples from Other States |
| Simplify enrollment and recertification processes. | Adopt practices and technologies that make it easier to apply, enroll, and recertify for WIC, such as:
| Review “Facilitating Enrollment,” “Documenting Eligibility,” and “Simplifying Certification” at https://www.cbpp.org/wiccertificationtoolkit See how state WIC agencies have adopted policy flexibilities at https://www.cbpp.org/wiccertificationpolicies Read the FNS memo, “Streamlining Certification Documentation Guidance,” at https://www.fns.usda.gov/wic/streamlining-certification-documentation-guidance Review “Streamlining and Modernizing WIC Enrollment” at https://www.cbpp.org/wiccasestudies |
| Offer telephone and/or videoconferencing appointments and remote options for nutrition education and breastfeeding support. | Provide options for certification and follow-up appointments by:
| Review “Additional WIC Flexibilities to Support Outreach, Innovation and Modernization Efforts through ARPA Nationwide Waivers – Supporting Remote WIC Operations” at https://www.fns.usda.gov/wic/flexibilities-support-outreach-innovation-and-modernization-efforts-through See “Scheduling Appointments” and “Phone/Video Appointments” at https://www.cbpp.org/wiccertificationtoolkit See “Section 2. VENA Approach — Participant-Centered and Health Outcome-Based” at https://wicworks.fns.usda.gov/sites/default/files/media/document/vena-guidance.pdf |
| Provide flexible scheduling with options for participants to easily reschedule appointments. | Offer:
| View the toolkit “Assessing Your WIC Certification Practices: Scheduling Appointments” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-appointments Review “Launching New Digital Tools for WIC Participants: A Guide for WIC Agencies” at https://www.cbpp.org/wicparticipanttechnology See “Section 3: WIC Clinic Experience” in “Making WIC Work Better” at https://frac.org/wp-content/uploads/Making-WIC-Work-Better-Full-Report.pdf |
| Ensure that appointments provide individualized nutrition information and excellent customer service. | Implement:
| See the FNS guidance “Value Enhanced Nutrition Assessment” at https://wicworks.fns.usda.gov/sites/default/files/media/document/vena-guidance.pdf and Vena Training Videos at https://wicworks.fns.usda.gov/resources/vena-training-videos See “WIC Nutrition Services Standards,” jointly developed by FNS and the National WIC Association, at https://wicworks.fns.usda.gov/resources/wic-nutrition-services-standards |
| Increase State Coordination Across Programs | ||
|---|---|---|
| Strategy | Implementation | Resources & Examples from States |
| Establish ongoing communication and coordination channels. | Work with other programs to:
| See how state WIC agencies are coordinating with Medicaid and SNAP at https://www.cbpp.org/wiccollaborationsurvey |
| Develop and implement cross-enrollment plans. | Work with program partners to plan, test, implement, monitor, and update cross-enrollment strategies. | See how state Medicaid agencies can automatically refer Medicaid applicants and enrollees to WIC and promote robust referrals by managed care organizations, health care providers, and community-based health workers at https://www.cbpp.org/medicaidwicopportunities See examples of cross-enrollment in New Mexico at https://thewichub.org/new-mexico-wic-and-snap-integration/ and in New Hampshire at https://thewichub.org/new-hampshire-wic-targeted-outreach-to-snap-and-medicaid-recipients/ |
| Build WIC referrals into SNAP and Medicaid enrollment processes and work with other state programs and organizations to develop streamlined referral processes. | Work with SNAP, Medicaid, and other programs and organizations to:
| See the toolkit “Assessing Your WIC Certification Practices: Coordinating Services” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-coordinating |
| Implement periodic data sharing with SNAP and Medicaid to measure coverage gaps and conduct targeted outreach. | Work with SNAP and Medicaid to:
| View the toolkits “Increasing WIC Coverage Through Cross-Program Data Matching and Targeted Outreach” at https://www.cbpp.org/wicdatamatchingtoolkit and “Assessing Your WIC Certification Practices: Targeting Outreach” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-targeting See how state agencies are coordinating with Medicaid and SNAP to reach WIC-eligible people at https://www.cbpp.org/wiccollaborationsurvey |
| Integrate WIC into multi-benefit applications. | Work with program partners and agency/department leadership to incorporate an automated referral to WIC for potentially eligible individuals when they complete an application for SNAP, Medicaid, and other programs. | See the toolkit “Assessing Your WIC Certification Practices: Facilitating Enrollment” at https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-enrollment Review the FNS policy, “Data Sharing to Improve Outreach and Streamline Certification in WIC,” at https://www.fns.usda.gov/wic/data-sharing Review “2023 WIC Technology Landscape Report” at https://media.nwica.org/2023%20wic%20tech%20report%204.5.23.pdf |
| Improve the Shopping Experience | ||
|---|---|---|
| Strategy | Implementation | Resources & Examples from States |
| Implement food package substitutions and flexibilities to respond to participant preferences. | Assess potential additions to the state’s authorized food list by:
| See the WIC food package regulations at https://www.ecfr.gov/current/title-7/section-246.10 Review “WIC Food Package Policy and Guidance” at https://wicworks.fns.usda.gov/sites/default/files/media/document/WIC%20Food%20Package%20Policy%20Guidance%20Mar2018_508c.pdf See “2022 Proposed Revisions to the WIC Food Packages” at https://www.fns.usda.gov/wic/wic-food-packages |
| Ensure that sufficient grocery stores are authorized for participants throughout the state and that all participants have access to an authorized store. | Assess the adequacy of authorized stores and address gaps by:
| See “Section 8: Optimizing the WIC Shopping Experience” in “Making WIC Work Better” at https://frac.org/wp-content/uploads/Making-WIC-Work-Better-Full-Report.pdf |
| Adopt and/or enhance apps to help participants locate authorized stores, view their food benefits, and identify WIC-eligible foods. | Engage participants in planning or revising a WIC app by:
| See data on WIC apps in the “Multi-state WIC Participant Satisfaction Survey: Learning from Program Adaptations during COVID” at https://thewichub.org/multi-state-wic-participant-satisfaction-survey-learning-from-program-adaptations-during-covid/ Review “The Association of WIC App Usage and Participant Redemption Outcomes” at https://healthyeatingresearch.org/wp-content/uploads/2021/05/HER-WIC-App-Usage-Brief-004.pdf Review “2023 WIC Technology Landscape Report” at https://media.nwica.org/2023%20wic%20tech%20report%204.5.23.pdf Review “Launching New Digital Tools for WIC Participants: A Guide for WIC Agencies” at https://www.cbpp.org/wicparticipanttechnology |
| Offer new shopping options like online ordering. | Assess the need for and feasibility of new options with input from participants, WIC-authorized stores, and the experience of other state WIC agencies and SNAP. | See “WIC Supports Online Shopping and Transactions” at https://www.fns.usda.gov/wic/supports-online-ordering-transactions Review “Blueprint for WIC Online Ordering Projects” at https://static1.squarespace.com/static/58a4dda16a49633eac5e02a1/t/60c8ea51296905287a9420eb/1623779922155/Blueprint+for+WIC+Online+Ordering.pdf |
| Assess State Policies and Priorities | ||
|---|---|---|
| Strategy | Implementation | Resources & Examples from States |
| Adopt available policy flexibilities for certification and program operations. | Periodically:
| View the toolkit “Assessing Your WIC Certification Practices” at https://www.cbpp.org/wiccertificationtoolkit See how state WIC agencies have adopted certification policy flexibilities at https://www.cbpp.org/wiccertificationpolicies Read the FNS memo, “Streamlining Certification Documentation Guidance,” at https://www.fns.usda.gov/wic/streamlining-certification-documentation-guidance |
| Support modernization of WIC technology and systems used for program applications, certification, and benefit delivery. | Take steps to:
| Review “2023 WIC Technology Landscape Report” at https://media.nwica.org/2023%20wic%20tech%20report%204.5.23.pdf See “FY 2023 WIC Modernization Grant —Notice of Funding Availability” at https://www.fns.usda.gov/wic/modernization-grant-nofa Review “Launching New Digital Tools for Participants: A Guide for WIC Agencies” at https://www.cbpp.org/wicparticipanttechnology |
| Ensure that the WIC funding allocated for local services is sufficient for staffing, facilities, and equipment to provide quality services. | Periodically review:
| See “WIC Nutrition Services and Administration Cost Study” at https://www.fns.usda.gov/wic/wic-nutrition-services-and-administration-nsa-cost-study |
End Notes
[1] This report was prepared with support from Linnea Sallack, an independent consultant formerly with the Altarum Institute and the California WIC program.
[2] Katie Bergh, Lauren Hall, and Zoë Neuberger, “About 2 Million Parents and Young Children Could Be Turned Away From WIC by September Without Full Funding,” CBPP, December 12, 2023, https://www.cbpp.org/research/food-assistance/about-2-million-parents-and-young-children-could-be-turned-away-from-wic.
[3]For more information on how WIC operates, see CBPP, “Policy Basics: Special Supplemental Nutrition Program for Women, Infants, and Children,” updated October 5, 2022, https://www.cbpp.org/cms/index.cfm?fa=view&id=5268.
[4]Steven Carlson and Zoë Neuberger, “WIC Works: Addressing the Nutrition and Health Needs of Low-Income Families for More Than Four Decades,” CBPP, updated January 27, 2021, www.cbpp.org/wicworks.
[5] USDA, Food and Nutrition Service, “National and State Estimates of WIC Eligibility and Program Reach in 2021,” November 2023, https://www.fns.usda.gov/research/wic/eligibility-and-program-reach-estimates-2021.
[6]Writing about pregnancy has often assumed cisgender identities, with the use of terms like “pregnant women.” Such language excludes people who are transgender or non-binary who give birth. In this report we attempt to be more inclusive by referring to pregnant people or using other non-gendered language wherever possible, while in places using gendered labels to avoid misrepresenting the data we are citing.
[7] People who are American Indian, Alaska Native, Asian, Native Hawaiian, Pacific Islander, or of multiple races had a coverage rate of 55.7 percent. Hispanic people, whom USDA refers to as “Hispanic/Latino,” may be of any race.
[8] WIC participation data going back several years are available at https://www.fns.usda.gov/pd/wic-program. Participation data do not include enrollees who have not obtained their food benefits.
[9] USDA WIC administrative data accessed December 2023, https://www.fns.usda.gov/pd/wic-program.
[10] See state fact sheets at www.cbpp.org/wiccoveragefactsheets.
[11]Organisation for Economic Co-operation and Development database on low birthweight and maternal mortality (OECD.Stat), accessed July 10, 2023, https://stats.oecd.org/. Per OECD.Stat, data will be published on OECD Data Explorer effective March 2024 (https://data-explorer.oecd.org/). See also Munira Z. Gunja, Evan D. Gumas, and Reginald D. Williams II, “U.S. Health Care from a Global Perspective, 2022: Accelerating Spending, Worsening Outcomes,” Commonwealth Fund, January 31, 2023, https://www.commonwealthfund.org/publications/issue-briefs/2023/jan/us-health-care-global-perspective-2022.
[12] Latoya Hill, Samantha Artiga, and Usha Ranji, “Racial Disparities in Maternal and Infant Health: Current Status and Efforts to Address Them,” Kaiser Family Foundation, November 1, 2022, https://www.kff.org/racial-equity-and-health-policy/issue-brief/racial-disparities-in-maternal-and-infant-health-current-status-and-efforts-to-address-them/. See also Hannah Katch, “State and Federal Policymakers Should Extend Postpartum Medicaid Coverage,” CBPP, August 27, 2020, https://www.cbpp.org/blog/state-and-federal-policymakers-should-extend-postpartum-medicaid-coverage.
[13] See Centers for Disease Control and Prevention, Department of Health and Human Services, “Pregnancy Mortality Surveillance System,” March 23, 2023, https://www.cdc.gov/reproductivehealth/maternal-mortality/pregnancy-mortality-surveillance-system.htm.
[14] Centers for Disease Control and Prevention, Department of Health and Human Services, “Racial and Ethnic Disparities in Pregnancy-Related Deaths — United States, 2007–2016,” September 6, 2019, https://www.cdc.gov/mmwr/volumes/68/wr/mm6835a3.htm.
[15] Infants born to American Indians and Alaska Natives are nearly twice as likely to die as infants born to white people. Infants born to Black people and to Native Hawaiians and other Pacific Islanders are over twice as likely to die as infants born to white people. See Hill, Artiga, and Ranji, op. cit.
[16] Hannah Katch, “Medicaid Expansion Improves Postpartum Coverage, Access to Care,” CBPP, October 21, 2020, https://www.cbpp.org/blog/medicaid-expansion-improves-postpartum-coverage-access-to-care.
[17] For more evidence on WIC’s effectiveness, see Carlson and Neuberger, op. cit. and Christine Borger et al., “WIC Infant and Toddler Feeding Practices Study 2 (ITFPS-2): Fifth Year Report,” USDA, June 2022, https://www.fns.usda.gov/resource/wic-infant-and-toddler-feeding-practices-study-2-itfps-2-fifth-year-report.
[18]See “Maternal and Child Health Outcomes Associated with the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC),” Agency for Healthcare Research and Quality, Department of Health and Human Services, April 19, 2022, https://www.fns.usda.gov/wic/maternal-and-child-health-outcomes.
[19] For a discussion of why food insecurity likely increased between 2021 and 2022 and racial disparities in food insecurity, see Lauren Hall, “Food Insecurity Increased in 2022, With Severe Impact on Households With Children and Ongoing Racial Inequities,” CBPP, October 26, 2023, https://www.cbpp.org/blog/food-insecurity-increased-in-2022-with-severe-impact-on-households-with-children-and-ongoing.
[20] Race and ethnicity for a household reflect the person in whose name the housing unit is owned or rented. Households of another race includes people who are American Indian, Alaska Native, Asian, Hawaiian, or Pacific Islander; their grouping, due to data limitations, may obscure higher rates of food insecurity for some subgroups. Hispanic people may be of any race. Matthew P. Rabbitt et al., “Household Food Security in the United States in 2022,” Economic Research Service, U.S. Department of Agriculture, October 2023, https://www.ers.usda.gov/publications/pub-details/?pubid=107702.
[21] CBPP analysis of 2022 Current Population Survey Food Security Supplement.
[22]See Steven Carlson and Joseph Llobrera, “SNAP Is Linked With Improved Health Outcomes and Lower Health Care Costs,” CBPP, December 14, 2022, https://www.cbpp.org/research/food-assistance/snap-is-linked-with-improved-health-outcomes-and-lower-health-care-costs; and Brynne Keith-Jennings, “Boosting SNAP: Benefit Increase Would Help Children in Short and Long Term,” CBPP, July 30, 2020, https://www.cbpp.org/blog/boosting-snap-benefit-increase-would-help-children-in-short-and-long-term.
[23] Elizabeth Metallinos-Katsaras et al., “A Longitudinal Study of WIC Participation on Household Food Insecurity,” Maternal and Child Health Journal, Vol. 15, July 2011, https://doi.org/10.1007/s10995-010-0616-5; Christopher E. Anderson et al., “Longer Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) Participation Duration Is Associated with Higher Diet Quality at Age 5 Years,” Journal of Nutrition, Vol. 152, Issue 8, August 2022, https://doi.org/10.1093/jn/nxac134; and Noura Insolera, Alicia Cohen, and Julia A. Wolfson, “SNAP and WIC Participation During Childhood and Food Security in Adulthood, 1984–2019,” American Journal of Public Health, Vol. 112, Issue 10, October 2022, https://doi.org/10.2105/AJPH.2022.306967.
[24] USDA estimated that 82 percent of WIC-eligible individuals with household income at or below 185 percent of the federal poverty guidelines participated in WIC in 2021. In light of issues with the underlying data and other findings, it seems likely that the actual coverage rate for this group is lower, but still well above participation by WIC-eligible individuals with household income above 185 percent of the federal poverty guidelines (who are only income-eligible for WIC if they are adjunctive eligibility by virtue of participating in Medicaid, SNAP, or TANF); USDA estimated that 5 percent of these individuals participated in WIC. USDA, Food and Nutrition Service, “National and State Estimates of WIC Eligibility and Program Reach in 2021.”
[25] Barbara Devaney, Linda Bilheimer, and Jennifer Schore, “Medicaid Costs and Birth Outcomes: The Effects of Prenatal WIC Participation and the Use of Prenatal Care,” Journal of Policy Analysis and Management, Vol. 11, No. 4, 1992, https://doi.org/10.2307/3324956.
[26] Roch A. Nianogo et al., “Economic evaluation of California prenatal participation in the Special Supplemental Nutrition Program for Women, Infants and Children (WIC) to prevent preterm birth,” Preventive Medicine, Vol. 124, July 2019, https://doi.org/10.1016/j.ypmed.2019.04.011.
[27] USDA WIC administrative data, op. cit.
[28] USDA, Food and Nutrition Service, “National and State Estimates of WIC Eligibility and Program Reach in 2021.”
[29] USDA, Food and Nutrition Service, “National and State Level Estimates of WIC Eligibility and Program Reach in 2019,” February 2022, https://www.fns.usda.gov/wic/national-state-level-estimates-eligibility-program-reach-2019.
[30] Puerto Rico’s coverage rate was 88.4 percent.
[31] For a more detailed discussion of state variation in WIC participation during the first year of the pandemic, see Lauren Hall and Zoë Neuberger, “Eligible Low-Income Children Missing Out on Crucial WIC Benefits During Pandemic,” CBPP, October 5, 2021, https://www.cbpp.org/research/food-assistance/eligible-low-income-children-missing-out-on-crucial-wic-benefits-during.
[32] USDA WIC administrative data, op. cit.
[33] USDA WIC administrative data, op. cit.
[34] In 2019, 92 percent of children eligible for Medicaid/CHIP participated. See KFF, “Medicaid/CHIP Child Participation Rates,” https://www.kff.org/medicaid/state-indicator/medicaidchip-child-participation-rates/. While data on SNAP take-up for children are not available, 82 percent of all eligible individuals participated in SNAP in 2019. See USDA, “SNAP Participation Rates by State, All Eligible People (FY 2019),” https://www.fns.usda.gov/usamap/2019.
[35] USDA, Food and Nutrition Service, “National and State Estimates of WIC Eligibility and Program Reach in 2021.”
[36] Sonya Schwartz, Zoë Neuberger, Jennifer Sullivan, Lauren Hall, and Elisabeth Burak, “State Medicaid Agencies Can Partner With WIC Agencies to Improve the Health of Pregnant and Postpartum People, Infants, and Young Children,” CBPP and Georgetown Center for Children and Families, December 20, 2023, Figure 2, https://www.cbpp.org/research/food-assistance/state-medicaid-agencies-can-partner-with-wic-agencies-to-improve-the.
[37] Zoë Neuberger and Lauren Hall, “WIC Coordination with Medicaid and SNAP,” CBPP, November 14, 2022, https://www.cbpp.org/research/food-assistance/wic-coordination-with-medicaid-and-snap-0.
[38] Jess Maneely and Zoë Neuberger, “Using Data Matching and Targeted Outreach to Enroll Families with Young Children in WIC,” CBPP, January 5, 2021, https://www.cbpp.org/research/food-assistance/using-data-matching-and-targeted-outreach-to-enroll-families-with-young.
[39] Bergh, Hall, and Neuberger, op. cit.
[40] USDA WIC administrative data and Bureau of Labor Statistics Consumer Price Index for All Urban Consumers for food at home. For more information on the increase in the fruit and vegetable benefit and its impact see https://www.fns.usda.gov/wic/2024-cash-value-voucher-benefit-amounts#:~:text=Based%20on%20recently%20enacted%20appropriations,subsequent%20actions%20impacting%20these%20amounts and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10469066/.
[41] Share Our Strength Center for Best Practices, “Early Childhood Research Brief: The Role of WIC,” https://bestpractices.nokidhungry.org/sites/default/files/media/wic-early-childhood-survey-brief_0.pdf; and Geraldine Henchy, “Making WIC Work Better: Strategies to Reach More Women and Children and Strengthen Benefits Use,” Food Research & Action Center, May 2019, https://www.frac.org/wp-content/uploads/Making-WIC-Work-Better-Full-Report.pdf.
[42]Zoë Neuberger and Lauren Hall, “State WIC Agencies Continue to Use Federal Flexibility to Streamline Enrollment,” CBPP, November 14, 2022, https://www.cbpp.org/research/food-assistance/state-wic-agencies-continue-to-use-federal-flexibility-to-streamline.
[43] See “Streamlining Certification Documentation” at https://www.fns.usda.gov/wic/streamlining-certification-documentation-guidance.
[44] Lorrene Ritchie et al., “Multi-state WIC Participant Satisfaction Survey: Learning from Program Adaptations during COVID,” National WIC Association, December 2021, https://media.nwica.org/nwamulti-state-wic-participant-satisfaction-surveynationalreportfinal.pdf.
[45] USDA published a proposed rule, “Special Supplemental Nutrition Program for Women, Infants and Children: Revisions in the Women, Infants and Children Food Packages,” on November 21, 2022. It includes increases in the cash-value benefit and new food package substitutions to accommodate participant preferences. If more flexibility is ultimately added to program rules, it will be even more important for states to make these options available to participants in meaningful ways. See https://www.regulations.gov/document/FNS-2022-0007-0001.
[46] Gretchen Swanson Center for Nutrition, “WIC Online Shopping Grant,” https://www.centerfornutrition.org/wic-online-ordering?rq=wic.
[47] USDA, Food and Nutrition Service, “Additional WIC Flexibilities to Support Outreach, Innovation, and Modernization Efforts through ARPA Nationwide Waivers – Supporting Remote WIC Operations,” February 1, 2023, https://www.fns.usda.gov/wic/flexibilities-support-outreach-innovation-and-modernization-efforts-through.
[48] A total of 66 states, Indian Tribal Organizations, and U.S. Territories received these grants. See USDA Food and Nutrition Service, “FY 2022 ARPA WIC Technology/Service Delivery Improvement: Communications, Data, and Metrics Grant,” updated November 17, 2023, https://www.fns.usda.gov/wic/technology-service-delivery-grant-summary.
[49] USDA, Food and Nutrition Service, “FY 2023 WIC Modernization Grant – Notice of Funding Availability,” May 22, 2023, https://www.fns.usda.gov/wic/modernization-grant-nofa.
[50]USDA is entering into a cooperative agreement with the Johns Hopkins Bloomberg School of Public Health, Benefits Data Trust, and the National WIC Association to oversee the grant process, provide technical assistance, and help evaluate state efforts. See USDA, Food and Nutrition Service, “FNS awards cooperative agreement to streamline enrollment in WIC through data matching,” https://www.fns.usda.gov/news-item/fns-016.23, and “FY 2023 WIC Enrollment via State-Level Referral Data Matching with SNAP and Medicaid,” 2023, https://www.fns.usda.gov/wic/data-sharing-rfa.
More from the Authors

Areas of Expertise

Areas of Expertise

Linnea Sallack is an independent consultant formerly with the Altarum Institute and the California WIC program.