State Medicaid Agencies Can Partner With WIC Agencies to Improve the Health of Pregnant and Postpartum People, Infants, and Young Children
Summary
Addressing the health-related social needs (HRSNs) of pregnant and postpartum people[2] and young children cannot wait. The U.S. continues to struggle with high rates of pregnancy-related deaths and infant mortality, particularly among people of color. Unmet needs, such as food insecurity, can undermine health and prevent parents and young children from thriving.
Both Medicaid and the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) — programs with shared goals and shared participants — can improve health during pregnancy, the postpartum period, and the early years of a child’s life — a high-stakes period of rapid family change.
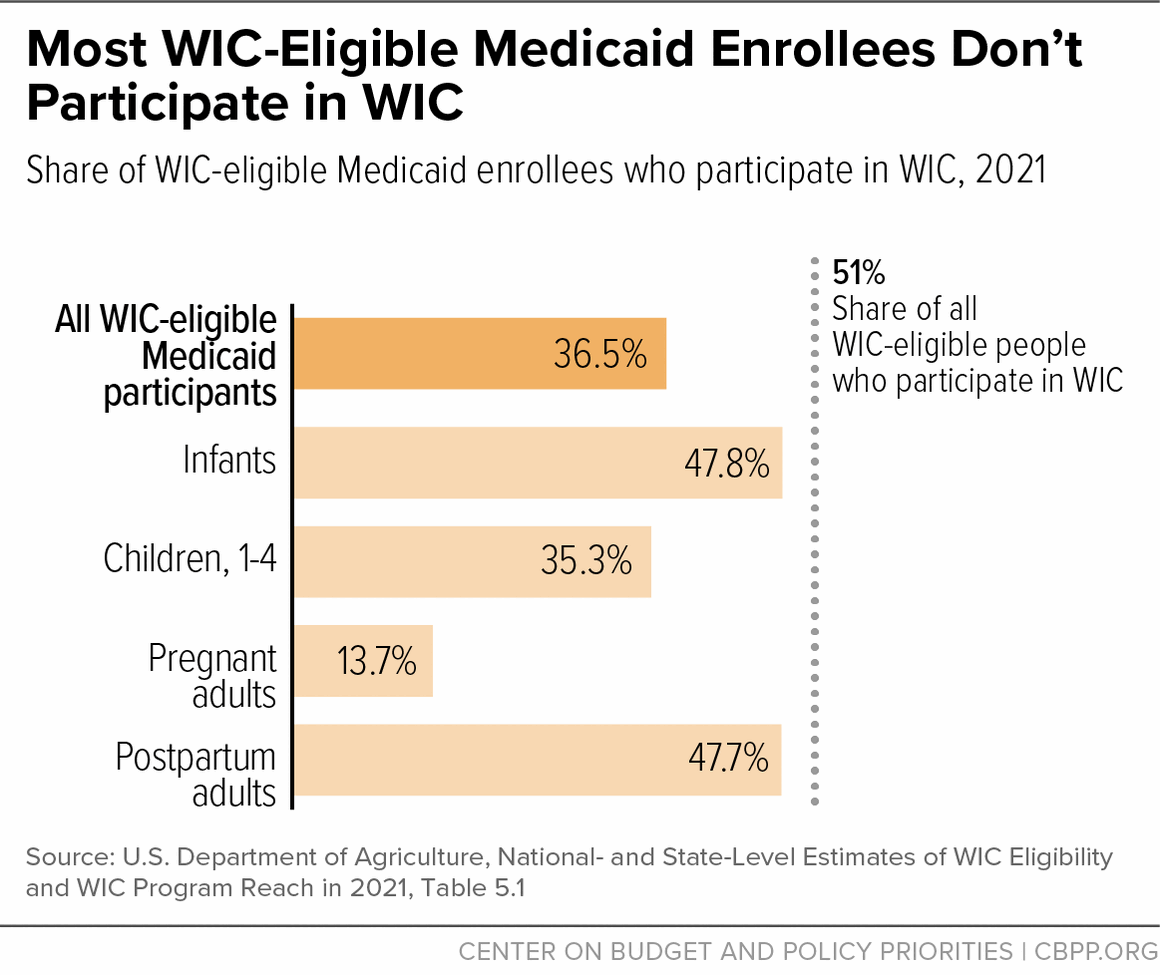
State Medicaid and WIC agencies can work together to increase WIC participation and improve the health of young children and parents nationwide. People who are enrolled in Medicaid are automatically income-eligible for WIC, and both programs reach a very large portion of the roughly 2 million infants who are eligible for both.[3] But while Medicaid reaches most eligible children and parents,[4] WIC reaches less than half of eligible pregnant people and young children. Moreover, only 37 percent of all WIC-eligible Medicaid enrollees participate in WIC and a meager 14 percent of WIC-eligible pregnant Medicaid enrollees participate.[5]
The climate is ripe for these agencies to work together. Congress recently enacted new Medicaid continuous coverage periods for pregnant people and children; connecting Medicaid enrollees to WIC can help ensure that they receive critical nutrition assistance and valuable services that can improve their health during this extended period of coverage. The Centers for Medicare & Medicaid Services (CMS) is also aligned with the goal of reducing food insecurity and, in negotiations with states, has been highlighting increasing WIC enrollment as a strategy to improve quality of care and address HRSNs. Meanwhile, as state Medicaid agencies embark on health and payment reforms focused on adults, they can also consider the time-sensitive needs of pregnant and postpartum people and young children.
States have a great deal of flexibility in the extent to which they coordinate between Medicaid and WIC. To enroll as many people who qualify for WIC as possible, states ideally would take advantage of every opportunity to connect Medicaid applicants and enrollees with WIC:
- Every Medicaid applicant who is pregnant, postpartum, or is a child under age 5 would be routinely and automatically referred to WIC.
- Medicaid enrollees who aren’t yet enrolled in WIC would be referred to WIC by state Medicaid agencies through a state data matching process that leads to direct WIC outreach.
- Then, as Medicaid enrollees obtain health care, managed care organizations (MCOs), health care providers, and community-based health workers would make robust referrals to WIC.
State Medicaid agencies can use the strategies described in this report to effectuate this vision:
- Share Medicaid enrollee data with WIC agencies to identify eligible families who are not enrolled in WIC, conduct targeted outreach to them, and simplify their enrollment. Large shares of WIC-eligible Medicaid enrollees nationwide are not participating in WIC, the U.S. Department of Agriculture (USDA) estimates. There are multiple ways to increase participation. When someone who is pregnant or postpartum applies for Medicaid, or when a caregiver applies for Medicaid for a child under 5, they can be automatically referred to WIC. States can also match Medicaid enrollee data with WIC data to conduct targeted WIC outreach directly to eligible Medicaid families who are not enrolled. In addition, states can strengthen the referral process by developing a standardized and streamlined referral mechanism that health care providers can use.
- Support a community-based health workforce that can strengthen connections to WIC. Community-based health workers — which can include community health workers (CHWs), doulas, home visitors, and case managers — can help mitigate food insecurity for pregnant and postpartum people and young children. They can conduct screenings for food insecurity, refer individuals to programs like WIC, and provide enrollment assistance and support in using WIC benefits. Medicaid can finance a community-based workforce in several ways, including through a “preventive services initiative”; directly as covered Medicaid services; through a Children’s Health Insurance Program (CHIP) Health Services Initiative; or by using administrative matching funds. States can also include requirements or incentives in Medicaid managed care contracts to build and define a community-based health workforce that can make linkages to WIC.
- Work with health care providers and Medicaid managed care organizations to include WIC enrollment as a strategy to improve quality and address HRSNs. Contracts with MCOs are a critical tool for shaping these efforts in most states. Medicaid can require MCOs to report on meeting WIC-related quality goals, enrollment goals, or both, and states can reward MCOs that improve. State agencies can also require MCOs to screen for and track HRSNs and make referrals to WIC and then can reward enrollment in WIC. MCOs can also be required to carry out “performance improvement projects” (PIPs) that include referrals to and enrollment in WIC as strategies to improve performance on both Maternal and Child Core Set quality measures.
By working together, state Medicaid agencies and WIC programs can improve the health of pregnant and postpartum people and very young children, potentially reducing racial disparities, and setting them on a path to better lifelong health.
Table of Contents
Momentum Is Building to Address Health-Related Social Needs Through Medicaid and WIC
Medicaid and WIC: Shared Goals, Shared Participants
New Medicaid Options Create Opportunities to Improve Enrollees’ Health by Enrolling Them in WIC
State Medicaid Agencies Can Share Data and Strengthen Referrals to Increase WIC Enrollment
Measuring and Tracking Progress on WIC Enrollment Among Medicaid Beneficiaries
Referring Medicaid Applicants to WIC
State Medicaid Agencies Can Support Community-Based Health Workers Who Strengthen Connections to WIC
Engage and Leverage WIC to Support the State’s Medicaid Quality Strategy
Incorporate WIC Into Efforts to Address Food Insecurity as a Health-Related Social Need
Momentum Is Building to Address Health-Related Social Needs Through Medicaid and WIC
Addressing health-related social needs (HRSNs), including food insecurity, of pregnant and postpartum people and young children, particularly those of color, is critical to building a healthy foundation for low-income families. HRSNs are an individual’s needs for social supports, such as housing or food security, that when not met may exacerbate poor health and quality of life outcomes. HRSNs are generally the result of underlying social determinants of health, or the conditions in which people are born, grow, work, and age.[6]
The rate of pregnancy-related deaths[7] in the U.S. tops the charts for developed nations, is more than double the rate of peer countries,[8] and is exceptionally high for Black people.[9] In addition, the infant mortality rate for Black infants was nearly double that of all infants, and the rates among American Indian and Alaska Native (AIAN) infants and Native Hawaiian or Other Pacific Islander infants were significantly higher than the average among all infants in 2022.[10] The COVID-19 pandemic cast a glaring light on health and social disparities stemming from racial inequities, with its disproportionate toll on people of color.[11] And food insecurity rose and racial disparities in food security widened in 2022, when 4.1 million more children lived in households experiencing food insecurity than in the previous year.[12] These factors, among others, have increased interest in addressing food insecurity and other HRSNs.[13]
Meanwhile, WIC, which provides nutritious foods, nutrition education, breastfeeding support, and referrals to health care and social services to low-income pregnant and postpartum people and children under age 5, is an underutilized resource that could help address food insecurity and, through referrals, other HRSNs. (See text box, “WIC Basics.”)
The share of eligible people participating in WIC has declined in the last decade, with only 51 percent of eligible individuals participating in 2021 and even smaller shares of pregnant people and children aged 1 through 4.[14] Underutilization of WIC is particularly alarming because WIC participation is associated with healthier babies who are more likely to survive infancy, improvements in pregnancy-related health outcomes — like reduced preeclampsia and weight gain — and better child health and development.[15] (See text box, “WIC Outcomes.”)
The Supplemental Nutrition Assistance Program (SNAP, formerly food stamps) also provides critical nutrition assistance to families with young children, and is associated with improved health outcomes. Research shows children in households participating in SNAP have reduced food insecurity (linked to fewer health and developmental risks), improved medication adherence, and less likelihood of developing heart disease or obesity as adults.[16] But this paper focuses on WIC because take-up of SNAP by eligible families with children, including those enrolled in Medicaid, is already robust. In addition, WIC provides services, such as breastfeeding support and nutrition counseling, that SNAP does not. Many other studies and analyses address linkages between Medicaid and SNAP, while fewer are focused on Medicaid and WIC.
Medicaid and WIC: Shared Goals, Shared Participants
Medicaid and WIC share the goal of improving health outcomes of pregnant and postpartum people and young children. Medicaid requires that all children receive comprehensive and preventive health care services including dental, mental health, developmental, and specialty services, known as Early and Periodic Screening, Diagnosis, and Treatment (EPSDT).[17] WIC provides food benefits and nutrition counseling tailored to the needs of pregnant and postpartum people and young children.
Medicaid requires states to have a plan for coordinating with the state WIC program, providing a timely annual written notice about the availability of WIC benefits (including the location and contact information for learning more), and referring pregnant and postpartum enrollees and children under 5 to their local WIC agency, but states determine how they will implement these requirements.[18]
Many people income-eligible for WIC get health coverage through Medicaid or CHIP. Indeed, Medicaid covers a large portion of all children and pregnant people in the U.S. It finances about 41 percent of total births, more than 60 percent of the births to Black and AIAN people, and more than half the births to Native Hawaiian or Other Pacific Islanders and Hispanic people.[19] In four states, Medicaid covers more than 50 percent of all births.[20]
WIC reaches nearly all infants who are eligible and about 4 in 10 babies born in the U.S. participate in WIC. But only 44 percent of eligible pregnant people and 43 percent of eligible children aged 1 through 4 participate in WIC.[21]
WIC participation by Medicaid enrollees, all of whom are adjunctively income-eligible for WIC, is even lower. Only 37 percent of all WIC-eligible Medicaid enrollees participate in WIC and a meager 14 percent of WIC-eligible pregnant Medicaid enrollees participate.[22] (See Figure 1.) Improving Medicaid’s connections to WIC is a promising approach to help more eligible pregnant and postpartum people, infants, and young children receive WIC benefits.
New Medicaid Options Create Opportunities to Improve Enrollees’ Health by Enrolling Them in WIC
Recent Medicaid changes reflect the importance of both postpartum coverage and stable eligibility for children. WIC can help maximize the potential of longer Medicaid coverage periods to ensure both postpartum people and infants get the health and nutrition services they need to thrive. The Consolidated Appropriations Act of 2022 (CAA)[23] included two important Medicaid eligibility changes.
First, it made permanent an option for states to lengthen postpartum coverage from the required 60 days to 12 months after the end of pregnancy. Nearly all states have implemented or are in various stages of implementing extended postpartum coverage.[24] States extending postpartum coverage to 12 months have an important, time-sensitive window of opportunity after a birth to reach and provide needed care and services to postpartum people and infants.[25]
Second, the CAA requires all states to provide 12-month continuous eligibility for children beginning in 2024.[26] This means that all children enrolled in Medicaid can remain enrolled for an entire year regardless of household changes. This also locks in a year of adjunctive WIC eligibility, so WIC can help maximize the potential of these longer coverage periods to ensure both postpartum people and infants get the health and nutrition services they need to thrive. Connecting more Medicaid-enrolled children to WIC would ensure they would benefit not only from a year of continuous health coverage, but a year of needed nutrition services as well.
Simultaneously, the Centers for Medicare & Medicaid Services (CMS) and the Food and Nutrition Service (FNS) are partnering to address HRSNs and reduce food insecurity. In an effort to increase WIC participation, CMS and FNS are encouraging state Medicaid and WIC agencies to regularly share data on the portion of Medicaid enrollees who are enrolled in WIC to conduct targeted WIC outreach and monitor changes over time. As part of this effort, FNS recently issued guidance about how to share data while complying with confidentiality provisions in both programs.[27]
In addition, FNS is using dedicated grant funding under the American Rescue Plan to increase take-up by launching innovative outreach strategies and modernizing the program to improve participants’ experience at WIC clinics and shopping for groceries with WIC benefits. This is the first time federal funding has been dedicated to this kind of WIC outreach. Among its strategies, USDA is encouraging state WIC agencies to use Medicaid and SNAP data to identify families who are eligible for WIC but not enrolled, conduct targeted outreach to them, and measure the effectiveness of this strategy to increase WIC take-up.[28] The first round of grants to state WIC agencies is slated to be announced by the end of January 2024, with awards made by the end of March 2024.
CMS guidance has detailed other ways in which Medicaid can support HRSNs,[29] including providing services such as case management and targeted case management that can help improve participation in other federal programs, including nutrition programs like WIC. (For more information about case management, see text box, “Types of Medicaid-Financed Community-Based Health Workers Helpful in Strengthening Connections to WIC.”)[30]
CMS is also signaling the importance of WIC participation by including a plan to track and improve participation in WIC as a condition of its approval of Section 1115 demonstrations that address nutrition supports in a number of states. These states, including Arkansas, Arizona, Massachusetts, New Jersey, Oregon, and Washington, are required to have a plan for tracking and increasing the share of Medicaid beneficiaries who are eligible for and enrolled in SNAP and WIC.[31]
Federal Policy Investments in Pregnancy-Related and Early Childhood Health and Nutrition Provide Additional Impetus for Action
The White House has developed national, cross-agency strategies that recognize that the U.S. health care system has a critical role to play in meeting all people’s nutritional needs.
The White House “Blueprint for Addressing the Maternal Health Crisis” includes a goal of strengthening economic and social supports for people before, during, and after pregnancy.[32] As a strategy for meeting this goal, it names the American Rescue Plan’s investments in WIC outreach, modernization, and innovation and pending updates to the program’s food package.[33] The blueprint also outlines that the Centers for Disease Control and Prevention, in partnership with states, territories, and local jurisdictions, will collect data on experiences before, during, and after pregnancy related to health and social disparities such as food security, as part of its Pregnancy Risk Assessment Monitoring System.[34]
Likewise, the White House Strategy on Hunger, Nutrition and Health includes integrating nutrition and health as one of its five pillars.[35] It encourages states to achieve 95 percent cross-enrollment of eligible people across SNAP, Medicaid, and other federal programs.[36] It also elevates the role that food security plays in overall health and plans to require universal screening for food insecurity in federal health care systems like the Veterans Administration and the Indian Health Service, because doing so can help practitioners recognize root causes that affect health and connect patients to resources like SNAP, WIC, or a local food bank.[37]
Most recently, the White House issued its U.S. Playbook to Address Social Determinants of Health, which it released alongside a companion “call to action” from HHS to health and social service stakeholders to address HRSNs.[38] The playbook describes the importance of collaboration across federal, state, and local governmental agencies; community-based organizations; health care providers; and other stakeholders to expand data gathering and sharing, support flexible funding for social needs, and support “backbone” organizations that manage cross-sector partnerships to improve health and well-being.
The White House encourages strategies including supporting expanded access to nutrition assistance through coordination with health programs. The HHS Call to Action recommends actions that health care providers, payers, community-based organizations, and public health departments can take to better address HRSNs, including making effective referrals to programs that address HRSNs (including WIC), leveraging the community-based workforce to connect people to programs and services, sharing data across sectors, and reporting on quality measures related to HRSNs.
State Medicaid Agencies Can Share Data and Strengthen Referrals to Increase WIC Enrollment
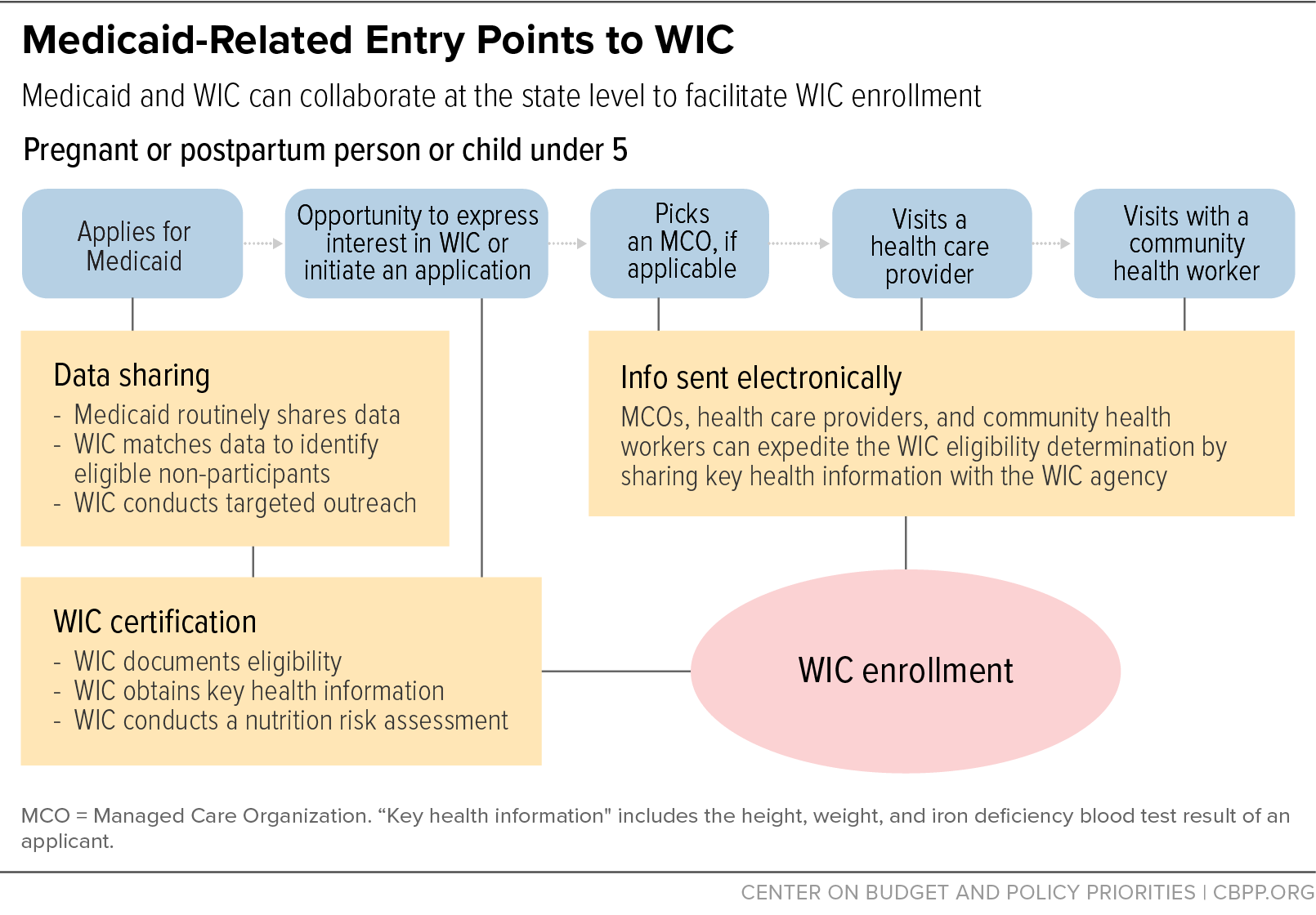
The portion of state Medicaid plans that addresses coordination with WIC should include a goal that Medicaid agencies will automatically refer to WIC every Medicaid applicant who is pregnant, postpartum, or under age 5. Ideally the state Medicaid agency would regularly share data with the WIC agency to use data matching to identify Medicaid enrollees who had not yet enrolled in WIC and conduct targeted outreach directly to them. Medicaid enrollees who weren’t yet participating in WIC would also be referred to WIC by managed care organizations (MCOs),[39] health care providers, and/or community-based health workers through a process that lets them share key information needed for WIC certification.
Collaboration between Medicaid and WIC at the state level allows for several important activities to put this kind of comprehensive approach into place, including sharing data to facilitate targeted WIC outreach, strengthening referrals, and measuring and tracking progress on enrollment among Medicaid beneficiaries in WIC. (See Figure 2.)
In recent years more state Medicaid and WIC programs have collaborated regularly, enabling robust implementation of Medicaid’s written notification and referral state plan requirements described above. Some have also entered into written cross-program agreements. These agreements sometimes let agencies share data that can be used to measure WIC take-up by Medicaid enrollees, conduct targeted outreach with streamlined enrollment, and measure progress over time.
As mentioned above, a WIC applicant who already has Medicaid coverage is automatically considered income-eligible for WIC and does not need to document their income to be enrolled.[40] Most states have an automated telephone- or web-based system that lets local WIC staff check whether a WIC applicant is adjunctively eligible.[41]
Generally, applicants who meet the income requirements have a medical or dietary condition that places them at nutritional risk, so a Medicaid enrollee is unlikely to be found ineligible for WIC. But WIC must collect the height, weight, and iron deficiency blood test results of applicants and conduct a nutrition risk assessment to tailor food benefits and nutrition counseling. Sometimes WIC staff obtain this information from health care providers, further streamlining WIC’s enrollment process, reducing duplicative measurements and bloodwork, and allowing WIC certification appointments to be completed by phone or through a video call instead of in person.[42]
Based on data gathered from state WIC programs in 2022, 28 WIC state agencies had a written agreement on coordination or data sharing with Medicaid and more were developing one. Eighteen WIC state agencies periodically (anywhere from daily to annually) received data on Medicaid enrollees and more were establishing processes to receive data.[43] Expanding the number of states with such agreements and practices, and making them more effective, could increase WIC take-up by eligible Medicaid enrollees.
Measuring and Tracking Progress on WIC Enrollment Among Medicaid Beneficiaries
USDA estimates that large shares of WIC-eligible Medicaid enrollees nationwide are not participating in WIC: 65 percent of Medicaid beneficiaries aged 1 through 4 and upwards of 86 percent of pregnant Medicaid enrollees do not participate in WIC.[44]
Likewise, individual states that have conducted data matches have found large enrollment gaps.[45] But states can design efforts to increase WIC take up by underserved groups by analyzing the gaps based on specific criteria — such as geography, WIC category (such as pregnant, postpartum, infant, or child aged 1 through 4), or race. States can also use data matching to establish a baseline measurement of the gap and measure progress over time, which would allow for an assessment of the effectiveness of efforts to increase WIC participation among Medicaid enrollees.
Referring Medicaid Applicants to WIC
When someone who is pregnant or postpartum applies for Medicaid, or when a caregiver applies for Medicaid for a child under 5, automatically referring them to WIC makes them aware of the program and gives them an opportunity to enroll.
For example, when someone applies for SNAP, Medicaid, and/or TANF in New Mexico they are automatically evaluated for WIC categorical eligibility, and referral information is sent to the WIC eligibility system, where it is linked to family records. WIC staff can access the information and follow up with applicants who are not already enrolled in WIC.[46] Between May 2022 and October 2023, this process resulted in an 18 percent increase in New Mexico’s WIC caseload.
If automatic referrals are not possible in a state, then online Medicaid applications could allow an applicant to initiate the WIC certification process online or request that relevant information be shared with the WIC program to begin the enrollment process.[47]
Conducting Targeted WIC Outreach
Analyzing which groups are more likely to be missing out on WIC allows states to tailor WIC outreach to underserved groups.[48] In 2022, 24 state agencies reported that they were using Medicaid enrollee data to reach underserved groups of WIC-eligible families, such as residents of particular counties, or children of certain ages, or pregnant people. Additional states were developing this capacity.
Matching Medicaid enrollee data with WIC enrollee data also allows state and local WIC agencies to conduct targeted WIC outreach directly to eligible families who are not enrolled. In 2022, ten states were using Medicaid data for targeted outreach — employing a combination of text messaging, phone calls, and mail — and additional states were preparing to conduct this kind of direct outreach. For example, the Minnesota Medicaid state agency shares data quarterly with the WIC state agency, which uses it to identify people who are eligible for WIC but not enrolled and to conduct targeted outreach via text messages that include a link to the online WIC application.[49]
Targeted outreach using text messaging has been successful in reaching and enrolling adjunctively eligible families in WIC.[50] States interested in launching similar efforts can learn how to effectively conduct data matches and targeted outreach from the states with experience, and federal funding will be available in 2024 to support such efforts.[50]
Strengthening Referrals
Referrals are more likely to be successful if WIC staff have the information they need to streamline the enrollment process. State-level data matching allows for automated referrals of large groups of WIC-eligible Medicaid enrollees. Working together, Medicaid and WIC state agencies can also develop a standardized statewide referral mechanism that health care providers can readily use.[52] As explained above, including height, weight, and iron deficiency blood test results in referrals streamlines WIC enrollment.[53] (See text box, “Information Useful for WIC Referrals.”) Health care providers could also facilitate prompt enrollment by allowing patients to complete WIC certification before or after health care appointments while pregnant, postpartum, or with an infant or young child, which could be accomplished by integrating a WIC video appointment into a health care visit or by co-locating WIC staff in the provider’s office.[54]
Patient information exchanges also offer a promising mechanism for facilitating referrals. These may be bidirectional exchanges between health care providers and WIC staff that allow for a closed-loop referral for patients, allowing the referring provider to find out if a patient has enrolled in WIC. Health care providers refer patients to WIC; WIC staff then use a designated process to follow up with the patient and to securely access patient health information needed for WIC enrollment. With participant consent, WIC can share the enrollment status of referred patients with their health care providers, thereby creating a closed-loop referral.
A number of states have statewide or local health information exchanges, health information organizations, or community information exchanges that could be used to facilitate a similar referral and enrollment process. Local entities in California have generated increased referrals and WIC enrollment through linkages with information exchanges.[55]
State Medicaid Agencies Can Support Community-Based Health Workers Who Strengthen Connections to WIC
Community-based health workers — which can include community health workers (CHWs), doulas, home visitors, and case managers — can help mitigate food insecurity for pregnant and postpartum people and young children. They can conduct screenings for food insecurity, refer individuals to programs like WIC, and provide enrollment assistance and support in using WIC benefits.
A community-based health workforce is also likely to include service providers who have shared lived experiences with the Medicaid enrollees they serve, and may be especially trusted and better able to communicate the value of programs like WIC and how to navigate them.[56](See text box, “Types of Medicaid-Financed Community-Based Health Workers Helpful in Strengthening Connections to WIC.”) Because the majority of Medicaid enrollees — 72 percent of all enrollees and 85 percent of children — receive their Medicaid coverage through a Medicaid managed care organization, policies to engage community-based health workers in WIC often require changes to a state’s managed care policies and/or contracts.[57]
States are drawing on community-based health workers to assess HRSNs like food insecurity and connect families to programs like WIC. North Carolina’s Department of Health and Human Services specifies that multidisciplinary care management teams, which can include CHWs, should assist patients in accessing and navigating social services, which may include WIC. The state has several other initiatives to address these needs such as a statewide, standardized screening tool that includes screening for food insecurity. Those with a given need can receive assistance in enrolling in programs like WIC and be provided closed-loop referrals to food and nutrition supports through an electronic statewide coordinated care network that gives community partners access to a resource directory, technology platform, and community engagement team.[58]
In Washington, a state law provided two years of grant funding to embed CHWs into care teams serving children from birth to 18 at seven primary care clinics. The CHWs will provide outreach, informal counseling, and serve as a liaison between health and social services.[59] While the grant does not require referrals to WIC, primary care clinics should encourage CHWs to make these connections for infants and young children. The state law also requires the state to explore permanent, statewide Medicaid reimbursement policies for CHWs.
Medicaid Financing of Community-Based Health Workers
Medicaid can finance a community-based workforce in a number of ways, including through a “preventive services initiative”; directly as covered Medicaid services; though a CHIP Health Services Initiative; or by using administrative matching funds. Regardless of the financing approach, states can use the Medicaid managed care contracting process to fund and provide incentives to managed care organizations to work with a community-based health workforce that screens for food insecurity and provides referrals and connections to WIC. Even if the Medicaid agency and MCOs make WIC referrals, people may still fall through the cracks, and community-based health workers can encourage families to apply to WIC and help them navigate the enrollment process.
Preventive Services Initiative
States can file a Medicaid state plan amendment (SPA) that allows unlicensed practitioners recommended by a physician or another licensed provider to provide preventive services.[60] The SPA could specify the role that community-based health workers will play in connecting Medicaid enrollees to WIC, which could include conducting screenings and providing referrals, enrollment assistance, and support to fully utilize WIC benefits. Several states have used SPAs to secure services provided by doulas,[61] CHWs, and home visiting programs.
- Maryland has a preventive services SPA that allows home visitors to provide services to pregnant and postpartum people, infants, and young children. These services can include “[f]acilitation of access to community or other resources that can improve birth-related outcomes such as … WIC.”[62]
- New Jersey allows doulas, recommended by a licensed practitioner, to provide services as part of its preventive services SPA.[63] While the SPA does not mention WIC, the doula’s scope of practice includes “assist[ing] members with community-based services that can improve health outcomes,” which may include programs like WIC.[64]
- Oregon also allows doulas supervised by licensed providers to provide services as part of its preventive services SPA, specifying the doula “facilitates and assures access to resources that can improve birth-related outcomes including … WIC [… and] SNAP ….”[65]
Financing “Covered Services”
States can also use SPAs to allow community-based health workers to provide certain covered services, including health education, health promotion and coaching, and care coordination or resource referral. Unless there is a Section 1115 demonstration, the benefits need to be offered statewide and without targeting specific populations, but states differ in the breadth of billable activity they allow under these categories.[66]
For example, Rhode Island covers community health worker services as a state plan prevention service. CHW-covered services include health promotion and coaching (which includes assessment and screening for HRSNs) as well as health system navigation and resource coordination (which can include helping beneficiaries access community resources).[67] While the state plan and provider manual do not specifically mention WIC, arranging a referral appointment with WIC would be an example of a “resource coordination” activity. In addition, CHWs can be reimbursed for “collateral services,” defined as “necessary activity not performed in the beneficiary’s presence, but benefitting the specific beneficiary,” which means that the work of arranging a referral appointment for an individual can be reimbursed even if it is done outside the presence of the beneficiary.
CHIP Health Services Initiatives (HSIs)
HSIs allow states to provide services focused on improving children’s health by using a limited amount of unspent CHIP funding. States receive the CHIP federal matching rate for HSIs, which is more generous than the Medicaid rate.[68] States implementing HSIs have flexibility to determine the type and scope of their initiative. Some HSIs address an ongoing need for the community generally, while others are more focused on a particular population or address acute public health issues. For example, in many states, an HSI is used to fund lead abatement[69] but it could also be used to train community-based health workers about food insecurity. It can focus on a particular group of people and does not have to be statewide as long as the initiative seeks to support children in families with low incomes.
An HSI can be used for any WIC-related approaches that improve health outcomes for children. Massachusetts has invested state funds in the WIC program since 1983. The state has also leveraged the CHIP HSI to optimize Medicaid reimbursement for WIC services.
In addition, New York uses this option to provide emergency food relief to food-insecure children through its Hunger Prevention Nutrition Assistance Program. While the program does not currently include WIC, services could be expanded to include referrals to services such as WIC. These examples demonstrate precedents for using HSIs to address food insecurity and the needs of WIC-eligible populations.
Medicaid Administrative Matching Funds
States receive federal matching funds for half the cost of most allowable Medicaid administrative expenditures.[70] Among other uses, states can claim administrative matching funds for recruitment, training, and workflow changes needed to integrate community-based health workers into the care team for pregnant and postpartum people and young children.
Using Medicaid Managed Care Contracting to Build and Shape a Community-Based Health Workforce That Can Make Linkages to WIC
States can include requirements or incentives in Medicaid managed care contracts to build and define a community-based health workforce that can make linkages to WIC. For plans that achieve sustained WIC enrollment, the state could provide preferential treatment, such as extra “points” in the managed care procurement process, a bump in payment, or “auto-assignment” in the plan when Medicaid enrollees do not choose a plan on their own.
As part of these contracts, states can build their workforce by requiring or providing incentives for plans to:
- Specify the scope of services and billing arrangements for a community-based health workforce, in collaboration with obstetric and pediatric primary care providers, to include food insecurity screenings and WIC referrals, including the cost of recruiting workers, training them, and integrating them into the care team.
- Provide a set ratio of trained community-based health workers to WIC-eligible members.
States can shape their community-based health workforce by requiring or providing incentives for plans to:
- Reimburse for a range of community-based health workers and specify how they are deployed and what they can do to help meet Medicaid goals.
- Prefer partnership with community-based organizations.
- Require community-based health workers to conduct screenings for HRSNs such as food insecurity and provide effective referrals to WIC.
- Train licensed providers to refer pregnant people, new parents, and children to the community-based health workforce.
- Provide Medicaid targeted case management services. A state first would have to opt to cover case management under the Medicaid state plan, and then community-based health workers could deliver the service to a specific population, such as pregnant and postpartum people and children under 5.[71] For example, most home visiting programs reimbursed by Medicaid are financed through this option.[72]
Some examples of states using these strategies to build and shape their workforces include:
- Michigan pays an incentive rate to plans that partner with local clinics or community-based organizations to build their community-based health workforce, rather than the plan hiring their own community-based health workers directly. Local community-based organizations and clinics are more likely to be culturally and linguistically competent, to have shared lived experiences, and to have built trust with community members, all enabling them to reach community members more effectively. To that end, Michigan also encourages plans to support health interventions led by CHWs, such as arranging for social services, which could include food assistance through WIC.[73]
- Illinois’ model contract requires MCOs to refer all pregnant enrollees to WIC and then during the third trimester to provide another referral to WIC to help prepare the pregnant person for the postpartum period and ensure continuity of care after the pregnancy.[74] After childbirth, the state requires MCOs to ensure that enrollees receive timely and evidence-based postpartum care, and to provide and document referrals to WIC, in addition to providing parenting classes and maternity education tools.
- Florida’s contract requires MCOs to refer eligible enrollees to WIC and provide the health information needed for WIC staff to enroll the person.[75]
- Massachusetts contractually requires its Medicaid MCOs and accountable care organizations to establish relationships with a provider or social service organizations that help eligible patients with identified food insecurity to enroll in WIC, provide the referral entity with information about the health-related social need, and follow up with the patient to ensure the need was met.[76]
- Oregon allows CHWs to provide certain Medicaid services under the supervision of a qualifying provider. These services can be delivered through Oregon’s Coordinated Care Organizations (CCOs)[77] or by fee-for-service Medicaid. [78] CCOs can allow “Traditional Health Workers” to provide health-related services such as screenings, health education, and assurance that people have access to the services they need.[79] Traditional health workers are defined as “trusted people from local communities who share socioeconomic ties and lived experience with Medicaid enrollees,” such as community health workers, peer support specialists, and doulas.[80]
Increasing WIC Participation Can Strengthen State Medicaid Agencies’ Efforts to Improve Quality and Address Health-Related Social Needs
WIC can further a state’s efforts to improve the quality of care that Medicaid provides to pregnant and postpartum people and young children. It can also address food insecurity as a health-related social need for these groups. Managed care is the primary way Medicaid delivers care to its enrollees, contracting with managed care organizations to deliver Medicaid benefits. As such, Medicaid MCOs are well-positioned to connect their members to WIC.
This section highlights tools that states can use — as part of the managed care contracting process — to prompt MCOs to include WIC referrals and coordination as part of broader Medicaid initiatives. Medicaid managed care contracts can encourage, provide incentives, or require MCOs to implement specific strategies to help identify and address HRSNs. Securing strong contract language can be an important first step toward ensuring that these needs, including food insecurity, are addressed, but monitoring and oversight are still important to achieving intended outcomes.
Engage and Leverage WIC to Support the State’s Medicaid Quality Strategy
Measuring whether services are being provided at all is an important first step in improving the quality of services.[81] It’s also a critical check on whether MCOs are providing required services and benefits. Metrics assess components that are integral to providing high-quality health care, including health systems, processes, outcomes, and patient perceptions.[82] To facilitate standardized reporting and comparison of performance across states, CMS has developed uniform sets of measures — or “Core Sets” — for state reporting; some Core Set reporting is required and other reporting remains voluntary.
Each year, CMS publishes sets of core measures showing the quality of care and health outcomes for adults participating in Medicaid[83] and children enrolled in CHIP.[84] To support its maternal and perinatal health-focused efforts and allow for more streamlined analysis and reports on maternal and perinatal health goals, CMS also issued a Maternity Core Set that includes measures from both the Adult and Child Core Sets that states may report.[85]
Increasing WIC participation has the potential to directly improve outcomes on three of the measures in the Child Core Set: reducing incidence of low birthweight,[86] increasing pediatric well visits in infancy and early childhood,[87] and boosting childhood immunizations.[88] Every state will be required to report to CMS on these measures, as well as the timeliness of prenatal care and postpartum care, starting in 2024 for all children under age 21 under the Child Core Set.[89]
Increases in WIC participation could also help states improve health outcomes on two measures from the Adult Core Set — prenatal and postpartum care and hemoglobin A1C control for patients with diabetes — but adult physical health measures remain optional for states to report. Table 1 describes each of these measures, the WIC feature that could improve performance, and evidence showing a link between WIC participation and improved outcomes.
Partnering with WIC might also help Medicaid improve quality in areas that are not formally measured by the Core Sets. For example, increasing enrollment in WIC can also help increase the number of people who receive body mass index assessments (used to assess whether a person’s weight could lead to health problems) and who receive nutrition and physical activity counseling. WIC can also create a feedback loop and strengthen accountability by referring WIC beneficiaries back to their health care provider for “interperiodic” (unscheduled) screenings that are required by EPSDT.[90]
| TABLE 1 | |||
|---|---|---|---|
| Federal Child, Maternal, and Adult Medicaid Quality Measures Align With WIC | |||
| Core Set Required Unless Indicated | Quality Measure | How Measure Aligns With WIC | How WIC Can Enhance Performance on the Measure |
| CHILD and MATERNAL | Well-Child Visits in First 30 Months of Life Child and Adolescent Well-Care Visits | WIC can reinforce that infants need frequent well-child visits according to periodicity schedule. WIC connects families to resources such as pediatric care and dental care. | A USDA study following children who enrolled in WIC as infants shows that nearly all (95 percent) have a doctor’s office, health clinic, or other medical facility that they visit for routine physical examinations and wellness checks around the time of the child’s 4th birthday.a |
| CHILD | Childhood Immunization Status | WIC screens the immunization records of children under age 2 and refers parents to immunization services to help ensure they are up to date. | Low-income children who have never participated in WIC have immunization rates ranging from 5 to 19 percent lower than current participants, while children who remain in WIC tend to have immunization rates comparable to higher-income children.b |
| CHILD and MATERNAL | Low Birthweight | WIC supports healthier pregnancies and births by providing the nutritious foods pregnant and postpartum participants need, referring them for essential medical care, and encouraging them to adopt behaviors associated with improved birth outcomes (such as not smoking). | Two studies report that mothers who participate in WIC show an 11 percent reduction in the incidence of small-for-gestational-age births. A third study found infants participating in WIC to be about 6 percent less likely to be low birthweight and 5 percent less likely to be small for gestational age. Another study found that Black mothers who participate in WIC are 5 percent less likely to deliver a low-birthweight infant and their infants are 5 percent less likely to be small for gestational age.c |
| CHILD | Weight Assessment and Counseling for Nutrition and Physical Activity for Children/ Adolescents | WIC supports healthy growth and weight among young children in several ways.d WIC conducts assessments of child weight and growth approximately every six months. WIC nutritionists, registered dietitians, or trained paraprofessionals meet with parents to provide nutrition counseling on child growth and healthy eating and physical activity practices for children. The fruits, vegetables, and whole grains in the food package are consistent with recommended food patterns associated with healthy weight. In addition, supporting higher breastfeeding rates among participating mothers may protect against excessive weight gain. | While evidence of overall progress in obesity prevention in recent years is mixed, there are some signs of progress in reducing obesity among young, low-income children. The prevalence of obesity among all children aged 2 to 5 years declined between 2004 and 2014, falling from 13.9 percent to 9.4 percent, before increasing back to 13.9 percent in 2016. Obesity rates among low-income children enrolled in WIC, however, have not risen. In one national study, children under 2 participating in WIC reported a decline from 2010 to 2014, with a flattening through 2018. Studies of national data on 2- to 4-year-old WIC participants have identified a flattening and decline in the prevalence of overweight and obesity from 2010 onward.e For example, one study found that obesity rates among low-income children 2 to 4 years of age fell from 15.9 percent in 2010 to 13.9 percent in 2016, with significant decreases in all age, sex, and racial/ethnic subgroups. Obesity rates among children participating in WIC fell in 36 states, the District of Columbia, and four territories over this period.f |
| CHILD, MATERNAL, and ADULT* | Timeliness of Prenatal Care and Postpartum Care | WIC connects families to resources such as pregnancy and postpartum care. | A study in California found that among low-income people, WIC participation was consistently associated with reduced risk of late entry (at six months pregnant or more) into prenatal care.g |
| ADULT* | Hemoglobin A1C Control for Patients with Diabetes | WIC provides counseling and referrals to help people manage gestational diabetes. It also provides pre- and postnatal nutrition education, which includes information about healthy eating during and after pregnancy, reading food labels when shopping, and cooking healthy meals. WIC also provides healthy foods such as fruits, vegetables, and whole grains. | There have been no studies examining improvements in Hemoglobin A1C control among WIC participants. The A1C test measures the average blood glucose levels over the past three months. But researchers have found, for example, a 17 percent reduction in preeclampsia and an 8 percent reduction in the number of women who gained more weight than recommended.h Reductions in preeclampsia and weight gain could be indicative of improved blood glucose levels. A study that examined overall diet quality during pregnancy found that WIC participants consuming the revised food package had a 2.38 point higher total Healthy Eating Index (HEI) score during pregnancy as compared with income-eligible non-WIC participants. The HEI assesses how well the diet aligns with the key recommendations of the Dietary Guidelines for Americans.i |
Require Medicaid MCOs to Report on Meeting WIC-Related Quality Goals, WIC Enrollment Goals, or Both — and Reward Improvement
States can use the Medicaid managed care contracting process to leverage WIC to improve quality and address food insecurity as an HRSN. However, Medicaid managed care contracts are renegotiated only once every several years, and states need to understand these tools as they prepare for their next negotiation.
States can — separately from CMS-mandated quality reporting metrics — require MCOs to report on meeting WIC enrollment goals or on the quality measures associated with WIC participation, and can reward MCOs that improve.[91] To address HRSNs, states can require MCOs to track data related to food insecurity and referrals to or enrollment in WIC. States can also require MCOs to screen for and track HRSNs, including food insecurity, and make referrals to WIC, and then reward enrollment in WIC. In addition, states can require MCOs to perform Medicaid “performance improvement projects” that include WIC to boost performance on certain quality measures.
States can begin by requiring MCOs to publicly report data for each of their Medicaid plans on the quality measures described in Table 1, which align with WIC, to aid in transparency and identify remaining gaps. States can then set benchmarks and use these metrics to track progress and compare among MCOs in their state or compare MCOs to those in neighboring states and the national average. In addition, states can require MCOs to publicly report on whether WIC enrollment goals are met.
State Medicaid agencies can also highlight for MCOs the link between WIC participation and quality improvements. For example, the Oregon Health Authority (Oregon’s Medicaid agency) highlighted the importance to Medicaid of relying on WIC to improve access to care and make quality care more accessible.[92] The Health Authority lists the metrics that offer a WIC collaboration opportunity and describes the WIC activities that support the metric. Oregon highlights that its Medicaid incentive metrics for Coordinated Care Organizations[93] — including childhood immunization status and timeliness of postpartum care — demonstrate an opportunity to collaborate with WIC to improve health outcomes.[94] The state also implemented a Social Determinants of Health Screening & Referral metric, which includes food security, in 2023.[95]
Medicaid payments could directly reward MCOs that meet WIC enrollment goals. Or Medicaid contracts can reward MCOs that meet goals associated with WIC participation, such as reducing the number of newborns with low birthweights. For example, in Pennsylvania, MCOs are eligible for bonus payments based on meeting the 75th or 90th percentile benchmark for quality metrics for prenatal care visits, postpartum care visits, and well-child visits in the first 15 months of life.[96]
Incorporate WIC Into Efforts to Address Food Insecurity as a Health-Related Social Need
CMS has issued guidance to support the goal of advancing health equity, ending hunger by 2030, and stemming increases in homelessness that occurred during the COVID pandemic.[97] Recent CMS policies allow state Medicaid agencies to provide support for both enrollment in WIC and receipt of WIC services in settings outside of traditional health care visits.
CMS’s 2021 guidance specifically mentions how Medicaid can connect people to other benefits that can address HRSNs, including “express lane” eligibility for nutrition programs, including WIC.[98]
In 2022, CMS provided a framework and additional considerations for states looking to address HRSNs through 1115 demonstrations. The framework encourages state Medicaid agencies to partner with other state agencies and social service providers to ensure enrollees experiencing food insecurity are connected to WIC (among other programs).[99] In exchange for new flexibility to cover nutrition and other services to help address HRSNs, states will have to follow guardrails designed to make sure that new investments in social needs spending don’t substitute for existing services or weaken investments in more traditional Medicaid services.
CMS’s 2023 guidance describes how states and MCOs can offer alternative services “in lieu of” services or settings described in the state plan to better address the social determinants of health and reduce costs.[100] Although the 2023 guidance doesn’t mention the federal nutrition programs by name, it refers to examples such as providing medically tailored meals for a target population as the type of services Medicaid could provide. CMS has also issued a proposed rule on how states can use “in lieu of” services in Medicaid managed care.[101]
The health sector, and Medicaid in particular, looks to primary care providers to connect people with services that can address HRSNs, including nutrition. In its vision for health equity, the White House encourages health care providers — including pediatricians, obstetricians, and gynecologists — to routinely conduct food security screenings and talk to patients about nutrition and physical exercise.[102] Share Our Strength (SOS) and the American Academy of Pediatrics (AAP) have committed to offering training to all 67,000 AAP members.[103] SOS has provided grants to state chapters of AAP to train pediatricians on how to both screen for nutrition security and refer patients to trusted resources.[104]
Both pediatric and pregnancy and postpartum provider organizations have embraced their role in addressing these needs, including food insecurity. AAP issued a formal policy statement highlighting the importance of collaboration between pediatricians and WIC.[105] Among its recommendations: pediatricians should disseminate information about WIC’s nutritional and educational benefits and work collaboratively with state and local WIC agencies and public health departments to coordinate services for children and maximize efforts to support breastfeeding.[106]
The American College of Obstetricians and Gynecologists recommends that providers inquire about and document HRSNs and maximize referrals to social services to help improve patients’ abilities to fulfill these needs.[107] The group also recommends that providers use “CommunityRx,” an evidence-based personalized referral system that connects patients to resources in their community to address HRSNs, including food insecurity and nutrition.[108]
Health care screenings offer an opportunity for providers to identify food insecurity and to refer patients to nutrition assistance programs, including WIC. In one example of a provider-led effort, a primary care pediatric clinic in North Carolina integrated WIC screening and referrals into the electronic health record and trained providers to use it. This resulted in a 40 percent increase in WIC enrollments in the co-located WIC site.[109] In addition, a Federally Qualified Health Center in Denver County partnered with WIC to have a WIC specialist co-enroll eligible Medicaid recipients in WIC during medical appointments.[110]
Require Medicaid MCOs to Screen for and Track HRSNs, Make Referrals to WIC, and Reward Enrollment in WIC
States can require that Medicaid MCOs screen and track HRSNs and, for example, reward MCOs that use a screening tool that identifies food insecurity and refers people who are food insecure to WIC, along with other nutrition assistance programs.
Screening for food insecurity can be simple. One recommended tool asks just two questions:[111]
1) Within the past 12 months, we worried whether our food would run out before we got money to buy more (Yes or No).
2) Within the past 12 months, the food we bought just didn’t last and we didn’t have money to get more (Yes or No).[112]
MCOs can then track HRSNs by capturing data related to family risk factors (such as food insecurity) and monitor how HRSNs are addressed (such as referrals to WIC or enrollment in WIC). One approach MCOs can use is to require providers to use “Z codes” (also called “V codes” in different classification systems) to document non-medical issues that affect a patient’s health.[113] These codes can be used to indicate risks, such as parent behavioral health diagnoses, recent family trauma, or food insecurity, that may rise to the level of warranting additional support for the child without a formal diagnosis. “Z codes” allow practitioners to address HRSNs by delivering or making referrals to specific services that may prevent, delay, or mitigate a later diagnosis for a child. Studies show that state policies play a role in the degree to which providers and health systems use these codes.[114]
State Medicaid agencies can then reward MCOs if health care providers conduct these screenings within a prescribed period, such as within 90 days of a person’s enrollment in the MCO, and if they then refer food insecure patients to WIC. MCOs could also potentially do the screenings themselves.
For example, North Carolina pays[115] MCOs as part of a care management per-member, per-month payment included in MCOs’ capitation rates to screen enrollees to assess HRSNs using an 11-question screening tool developed in multiple languages.[116] A “yes” response to any question sets in motion assistance with enrolling in programs like SNAP or WIC and connection to a statewide coordinated care network to electronically link people with identified needs to community resources and allow for feedback on the outcome of that connection.[117]
Require Medicaid MCOs to Implement Medicaid Performance Improvement Projects That Include WIC Enrollment
States that operate Medicaid managed care programs must have a written quality strategy that includes “performance improvement projects” (PIPs) to improve access, quality, or timeliness of care.[118] States can require MCOs to carry out PIPs that include referrals and enrollment in WIC as strategies to improve performance on both Maternal and Child Core Set quality measures. In recent years, a number of PIPs have focused on improvements in pregnancy, [119] postpartum, and child health.
For example, Tennessee requires its MCOs to implement PIPs related to child or perinatal health.[120]Minnesota’s 2021 to 2023 PIP focus is Healthy Start for Mothers and Their Children (for the Families and Children contract).[121]Wisconsin’s 2023 Medicaid managed care contract requires all MCOs to conduct a performance improvement project to identify and reduce health care disparities, including narrowing disparities in postpartum care.[122] A PIP could also require MCOs to report on WIC-related quality metrics to help identify remaining gaps. States can then reward MCOs financially if the measures improve by established amounts, or if WIC enrollment grows by a certain amount.
End Notes
[1] This report was prepared with support from Sonya Schwartz, an independent consultant. It draws heavily on an earlier paper written by Donna Cohen Ross, an independent consultant, for the Center on Budget and Policy Priorities.
[2] Writing about pregnancy has often assumed cisgender identities, with the use of terms like “pregnant women.” Such language excludes people who are transgender or non-binary who give birth. In this report we attempt to be more inclusive by referring to pregnant people or using other non-gendered language wherever possible, while in places using gendered labels to avoid misrepresenting the data or quality measures we are citing.
[3] Other eligibility requirements are described in the text box “WIC Basics.”
[4] Jennifer M. Haley et al., “Uninsurance Rose Among Children and Parents in 2019,” Urban Institute, July 2021, https://www.urban.org/sites/default/files/publication/104547/uninsurance-rose-among-children-and-parents-in-2019.pdf.
[5] Food and Nutrition Service, U.S. Department of Agriculture, “National and State Estimates of WIC Eligibility and Program Reach in 2021,” November 2023, Table 5.1, https://www.fns.usda.gov/research/wic/eligibility-and-program-reach-estimates-2021.
[6] Elizabeth Hinton, “A Look at Recent Medicaid Guidance to Address Social Determinants of Health and Health-Related Social Needs,” KFF, February 22, 2023, https://www.kff.org/policy-watch/a-look-at-recent-medicaid-guidance-to-address-social-determinants-of-health-and-health-related-social-needs/.
[7] This piece uses the term “pregnancy-related deaths” even if the underlying study used the term “maternal deaths.”
[8] The White House, “White House Blueprint For Addressing The Maternal Health Crisis,” June 2022, https://www.whitehouse.gov/wp-content/uploads/2022/06/Maternal-Health-Blueprint.pdf.
[9] The maternal mortality rate is three times higher for Black women than for white women. See the Commonwealth Fund, “The U.S. Maternal Mortality Crisis Continues to Worsen: An International Comparison,” December 1, 2022, https://www.commonwealthfund.org/blog/2022/us-maternal-mortality-crisis-continues-worsen-international-comparison.
[10] Danielle M. Ely and Anne K. Driscoll, “Infant Mortality in the United States: Provisional Data From the 2022 Period Linked Birth/Infant Death File,” National Center for Health Statistics, November 2023, https://www.cdc.gov/nchs/data/vsrr/vsrr033.pdf.
[11] AIAN and Hispanic people have had a higher risk for COVID-19 infection, and AIAN, Hispanic, and Black people have had a higher risk for hospitalization and death due to COVID-19. These are cumulative and age-adjusted data from April 2020 to October 2022. Latoya Hill, Samantha Artiga, and Mambi Ndugga, “COVID-19 Cases, Deaths and Vaccinations by Race/Ethnicity as of Winter 2022,” KFF, March 7, 2023, Figure 1, https://www.kff.org/coronavirus-covid-19/issue-brief/covid-19-cases-deaths-and-vaccinations-by-race-ethnicity-as-of-winter-2022/.
[12] Lauren Hall, “Food Insecurity Increased in 2022, With Severe Impact on Households With Children and Ongoing Racial Inequities,” CBPP, October 26, 2023, https://www.cbpp.org/blog/food-insecurity-increased-in-2022-with-severe-impact-on-households-with-children-and-ongoing.
[13] In addition, the National Governor’s Association issued a playbook on “Tackling the Maternal and Infant Health Crisis.” See National Governors Association, “Maternal and Infant Health,” https://www.nga.org/maternal-infant-health/.
[14] Food and Nutrition Service, U.S. Department of Agriculture, “National and State Level Estimates of WIC Eligibility and Program Reach in 2020,” updated January 9, 2023, https://www.fns.usda.gov/wic/eligibility-and-program-reach-estimates-2020.
[15] Steven Carlson and Zoë Neuberger, “WIC Works: Addressing the Nutrition and Health Needs of Low-Income Families for More Than Four Decades,” CBPP, updated January 27, 2021, https://www.cbpp.org/research/food-assistance/wic-works-addressing-the-nutrition-and-health-needs-of-low-income-families
[16] Steven Carlson and Joseph Llobrera, “SNAP Is Linked With Improved Health Outcomes and Lower Health Care Costs,” CBPP, December 14, 2022, https://www.cbpp.org/research/food-assistance/snap-is-linked-with-improved-health-outcomes-and-lower-health-care-costs.
[17] Centers for Medicaid & Medicare Services, “Early and Periodic Screening, Diagnostic, and Treatment,” https://www.medicaid.gov/medicaid/benefits/early-and-periodic-screening-diagnostic-and-treatment/index.html.
[18] The Social Security Act at 1902(a)(11)(C) and 1902(a)(53) requires Medicaid to notify all pregnant or breastfeeding people and young children of the availability of the benefits of WIC and to coordinate vaccinations with WIC. Medicaid regulations at 42 C.F.R. § 431.635 implement these requirements. In addition, the regulation specifies that Medicaid must effectively inform individuals who are blind or deaf or who cannot read or understand the English language.
[19] Michelle J.K. Osterman et al. “Births: Final Data for 2021,” Centers for Disease Control and Prevention, January 31, 2023, https://www.cdc.gov/nchs/data/nvsr/nvsr72/nvsr72-01.pdf.
[20] The four states are Louisiana, Mississippi, New Mexico, and Oklahoma. See KFF, “Births Financed by Medicaid,” 2021, https://www.kff.org/medicaid/state-indicator/births-financed-by-medicaid/?currentTimeframe=0&sortModel=%7B%22colId%22:%22Percent%20of%20Births%20Financed%20by%20Medicaid%22,%22sort%22:%22desc%22%7D.
[21] Food and Nutrition Service, U.S. Department of Agriculture, “National and State Level Estimates of WIC Eligibility and Program Reach in 2021,” November 2023, https://www.fns.usda.gov/research/wic/eligibility-and-program-reach-estimates-2021.
[22] Ibid., Table 5.1.
[23] Consolidated Appropriations Act, 2022, H.R. 2471, https://www.congress.gov/bill/117th-congress/house-bill/2471/text.
[24] KFF, “Medicaid Postpartum Coverage Extension Tracker,” September 21, 2023, https://www.kff.org/medicaid/issue-brief/medicaid-postpartum-coverage-extension-tracker/.
[25] By law, infants born to Medicaid enrollees are automatically covered until the child turns 1, but this option can help ensure that postpartum people also receive health care services in this important time period.
[26] Currently, 23 states provide continuous eligibility to children in Medicaid. The CAA requirement will bring the remaining 27 states and the District of Columbia in line. See KFF, “State Adoption of 12-Month Continuous Eligibility for Children’s Medicaid and CHIP,” January 1, 2023, https://www.kff.org/health-reform/state-indicator/state-adoption-of-12-month-continuous-eligibility-for-childrens-medicaid-and-chip.
[27] Food and Nutrition Service, USDA, “WIC Policy Memorandum #2023-5: Data Sharing to Improve Outreach and Streamline Certification in WIC,” April 25, 2023, https://www.fns.usda.gov/wic/data-sharing.
[28] USDA is entering into a cooperative agreement with the Johns Hopkins Bloomberg School of Public Health, Benefits Data Trust, and the National WIC Association to oversee the grant process, provide technical assistance, and help evaluate state efforts. See Food and Nutrition Service, “FNS awards cooperative agreement to streamline enrollment in WIC through data matching,” https://www.fns.usda.gov/news-item/fns-016.23, and “FY 2023 WIC Enrollment via State-Level Referral Data Matching with SNAP and Medicaid,” 2023, https://www.fns.usda.gov/wic/data-sharing-rfa.
[29] CMS, CMCS Informational Bulletin, “Coverage of Services and Supports to Address Health-Related Social Needs in Medicaid and the Children’s Health Insurance Program,” November 16, 2023, https://www.medicaid.gov/sites/default/files/2023-11/cib11162023.pdf; CMS, “Coverage of Health-Related Social Needs (HRSN) Services in Medicaid and the Children’s Health Insurance Program (CHIP): November 2023,” https://www.medicaid.gov/sites/default/files/2023-11/hrsn-coverage-table.pdf; CMS, “Addressing Health-Related Social Needs in Section 1115 Demonstrations,” December 6, 2022, https://www.medicaid.gov/sites/default/files/2023-01/addrss-hlth-soc-needs-1115-demo-all-st-call-12062022.pdf; Anne Marie Costello, Letter to State Health Officials, SHO# 21-001 RE: Opportunities in Medicaid and CHIP to Address Social Determinants of Health (SDOH), January 7, 2021, https://www.medicaid.gov/federal-policy-guidance/downloads/sho21001.pdf.
[30] An in-depth discussion of state options to address HRSNs through Medicaid is forthcoming from CBPP’s Allison Orris, Anna Bailey, and Jennifer Sullivan, titled “States Have Flexibility to Use Medicaid to Address Health-Related Social Needs.”
[31] Danielle Daly, Letter to Dawn Stehle, Arkansas Department of Human Services, December 28, 2022, https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/ar-arhome-demo-appvl-12282022.pdf; Daniel Tsai, Letter to Carmen Heredia, Arizona Healthcare Cost Containment System, June 7, 2023, https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/az-coid-chip-demonstn-aprl-ca.pdf; Angela Garner, Letter to Mike Levine, Executive Office of Health and Human Services, June 21, 2023, https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/ma-masshealth-apprvl-06212023.pdf, Chiquita Brooks La-Sure, Letter to Jennifer Jacobs, Division of Medical Assistance and Health Services, March 30 2023, https://www.medicaid.gov/medicaid/section-1115-demonstrations/downloads/nj-1115-cms-exten-demnstr-aprvl-03302023.pdf; Daniel Tsai, Letter to Charissa Fotinos, Washington Health Care Authority, June 30, 2023, https://www.medicaid.gov/sites/default/files/2023-06/wa-medicaid-transformation-ca-06302023.pdf; Daniel Tsai, Letter to Dana Hittle, Oregon Health Authority, April 20, 2023, https://www.medicaid.gov/sites/default/files/2023-04/or-health-plan-ca-04202023.pdf.
[32] The White House, “White House Blueprint For Addressing The Maternal Health Crisis,” June 2022, https://www.whitehouse.gov/wp-content/uploads/2022/06/Maternal-Health-Blueprint.pdf.
[33] The White House, June 2022, see section 5.1, pp. 51-52.
[34] The White House, June 2022, see section 3.1, p. 38.
[35] The White House, “Biden-Harris Administration National Strategy on Hunger, Nutrition, and Health,” September 2022, https://www.whitehouse.gov/wp-content/uploads/2022/09/White-House-National-Strategy-on-Hunger-Nutrition-and-Health-FINAL.pdf
[36] The White House, September 2022, p. 16.
[37] The White House, September 2022, p. 19.
[38] The White House, “U.S. Playbook to Address Social Determinants of Health,” November 2023, https://www.whitehouse.gov/wp-content/uploads/2023/11/SDOH-Playbook-3.pdf; HHS, “Call to Action: Addressing Health-Related Social Needs in Communities Across the Nation,” November 2023, https://aspe.hhs.gov/sites/default/files/documents/3e2f6140d0087435cc6832bf8cf32618/hhs-call-to-action-health-related-social-needs.pdf.
[39] The majority of Medicaid enrollees — 72 percent of all enrollees and 85 percent of children — receive their Medicaid coverage through a Medicaid managed care organization. Medicaid and CHIP Payment and Access Commission (MACPAC), “Exhibit 30. Percentage of Medicaid Enrollees in Managed Care by State and Eligibility Group,” December 2023, https://www.macpac.gov/publication/percentage-of-medicaid-enrollees-in-managed-care-by-state-and-eligibility-group/.
[40] Recipients of SNAP and monthly TANF cash assistance payments are also adjunctively eligible for WIC. For more details about the adjunctive eligibility rules, see 7. C.F.R. § 246.7 (d)(2)(vi), https://www.law.cornell.edu/cfr/text/7/246.7.
[41] States with such automated systems do not necessarily have a written agreement in place and do not need to receive batches of data to check applicants’ adjunctive eligibility. For more information about each state’s practices for checking for adjunctive eligibility, see Zoë Neuberger and Lauren Hall, “State WIC Agencies Continue to Use Federal Flexibility to Streamline Enrollment,” CBPP, updated November 14, 2022, Table 1, www.cbpp.org/wiccertificationpolicies.
[42] Long-standing federal rules require applicants to be present during certification appointments, with exceptions for newborn infants, children with working parents, and individuals with health conditions that prevent them from attending in-person appointments. (See 7 C.F.R. § 246.7(o).) Under federal waivers provided during the pandemic, WIC agencies switched to conducting appointments by telephone or videoconference, and did not have to collect anthropometric information. Under American Rescue Plan authority, these waivers have been extended through September 2026, but WIC agencies must now collect anthropometric information. See Food and Nutrition Service, U.S. Department of Agriculture, “Flexibilities to Support Outreach, Innovation, and Modernization,” August 4, 2023, https://www.fns.usda.gov/wic/modernization/flexibilities. Receiving that information from health care providers eliminates the need for an appointment at a WIC clinic.
[43] For state-by-state information, see Zoë Neuberger and Lauren Hall, “WIC Coordination With Medicaid and SNAP,” updated November 14, 2022, www.cbpp.org/wiccollaborationsurvey.
[44] U.S. Department of Agriculture, “National- and State-Level Estimates of WIC Eligibility and WIC Program Reach in 2021,” Table 5.1, https://fns-prod.azureedge.us/sites/default/files/resource-files/wic-eligibility-report-vol1-2021.pdf.
[45] See Jess Maneely and Zoë Neuberger, “Using Data Matching and Targeted Outreach to Enroll Families With Young Children in WIC,” CBPP and Benefits Data Trust, January 5, 2021, Figure 1, www.cbpp.org/wicpilotreport.
[46] National WIC Association, “New Mexico WIC and SNAP Integration,” December 16, 2022, https://thewichub.org/new-mexico-wic-and-snap-integration/.
[47] For more information about how to incorporate WIC into an online application, see CBPP, “Assessing Your WIC Certification Practices,” https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#question-enrollment-3.
[48] For example, Kansas’s Medicaid agency used SNAP data to conduct WIC outreach in communities with significant Black, Latino, and Native American populations who face disparate levels of food insecurity. American Public Human Services Association, “Kansas Spotlight: Forming Connections Between SNAP and WIC to Tackle Food Insecurity,” https://files.constantcontact.com/391325ca001/90c636ac-96e1-4cc5-8e2b-f62af781fdda.pdf.
[49] For more information see National WIC Association, “Minnesota WIC Data Matching and Targeted Outreach,” November 21, 2022, https://thewichub.org/minnesota-wic-data-matching-and-targeted-outreach/.
[50] For results of pilots conducted in Colorado, Massachusetts, Montana, and Virginia, see Jess Maneely and Zoë Neuberger, “Targeted Text Message Outreach Can Increase WIC Enrollment, Pilots Show,” Benefits Data Trust and CBPP, June 10, 2021, www.cbpp.org/wictexting.
[51] For planning tools and resources on how to launch data matching and targeted outreach, see CBPP and Benefits Data Trust, “Toolkit: Increasing WIC Coverage Through Cross-Program Data Matching and Targeted Outreach,” March 1, 2022, www.cbpp.org/wiccrossenrollmenttoolkit. For information on which states are conducting targeted outreach, see Zoë Neuberger and Lauren Hall, “ WIC Coordination With Medicaid and SNAP,” updated November 14, 2022, Table 1, www.cbpp.org/wiccollaborationsurvey. For information on federal funding see Food and Nutrition Service, USDA, “FNS awards cooperative agreement to streamline enrollment in WIC through data matching,” September 21, 2023, https://www.fns.usda.gov/news-item/fns-016.23#:~:text=The%20Bloomberg%20School%20and%20its%20collaborators%2C%20Benefits%20Data%20Trust%20and,of%20other%20federal%20programs%20like. For more information on when federal funding is likely to be available, see Food and Nutrition Service, USDA, “FY 2023 WIC Enrollment via State-Level Referral Data Matching with SNAP and Medicaid,” 2023, p. 16, available at https://www.grants.gov/search-results-detail/347786.
[52] For example, Colorado has developed an online WIC referral form that is promoted to health care providers so they can refer patients directly to WIC. Colorado Department of Public Health and Environment, “Colorado WIC Families- Referral Form,” https://www.healthinformatics.dphe.state.co.us/WICSignUp.
[53] For example, New Jersey’s WIC program has developed a referral form for providers that allows them to share the anthropometric information needed for WIC nutrition risk assessments. New Jersey WIC, “New Jersey WIC Health Care Referral,” https://www.state.nj.us/health/forms/wic-41.pdf.
[54] For more suggestions on how WIC and health care providers can coordinate services, see CBPP, “Assessing Your WIC Certification Practices,” https://www.cbpp.org/research/food-assistance/assessing-your-wic-certification-practices#questions-coordinating.
[55] See Santa Cruz County’s Serving Communities Health Information Organization project, California WIC Association, “Santa Cruz Multi-Partner Linkage Supports WIC Referrals and Enrollment,” https://www.calwic.org/wp-content/uploads/2023/06/Community-Bridges-and-SCHIO-Summary.pdf, and San Francisco Department of Public Health’s electronic health records project, “San Francisco WIC Linkage with Epic Electronic Health Record System,” https://www.calwic.org/wp-content/uploads/2023/06/San-Francisco-Summary.pdf. In these projects the WIC agency indicates when a referral has been received but not whether the individual has been enrolled in WIC.
[56] Carmen L. Green et al., “The Cycle to Respectful Care: A Qualitative Approach to the Creation of an Actionable Framework to Address Maternal Outcome Disparities,” International Journal of Environmental Research and Public Health, May 6, 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8141109/.
[57] Medicaid and CHIP Payment and Access Commission, “Exhibit 30. Percentage of Medicaid Enrollees in Managed Care by State and Eligibility Group,” December 2023, https://www.macpac.gov/publication/percentage-of-medicaid-enrollees-in-managed-care-by-state-and-eligibility-group/.
[58] North Carolina of Health and Human Services, “Healthy Opportunities,” https://www.ncdhhs.gov/about/department-initiatives/healthy-opportunities and “NCCARE360,” https://www.ncdhhs.gov/about/department-initiatives/healthy-opportunities/nccare360.
[59] Washington Health Care Authority, “Community Health Worker (CHW) Grant,” https://www.hca.wa.gov/about-hca/programs-and-initiatives/clinical-collaboration-and-initiatives/community-health-worker-chw-grant.
[60] Preventive Services Initiatives, defined in federal regulation (42 CFR 440.130(c)) and law (Social Security Act 1905(a)(13), and Cindy Mann, “Update on Preventive Services Initiatives,” CMS Center for Medicaid & CHIP Services, November 27, 2013, https://www.medicaid.gov/sites/default/files/federal-policy-guidance/downloads/CIB-11-27-2013-Prevention.pdf. .
[61] Tomás Guarnizo, “Doula Services in Medicaid: State Progress in 2022,” Center for Children and Families, Georgetown University, June 2, 2022, https://ccf.georgetown.edu/2022/06/02/doula-services-in-medicaid-state-progress-in-2022/.
[62] Ruth A. Hughes, Letter to Tricia Roddy, Maryland Department of Health, June 15, 2022, https://www.medicaid.gov/medicaid/spa/downloads/MD-22-0005.pdf.
[63] New Jersey recently reported low use of doula services, which began in 2021, and attributed it to lack of awareness among Medicaid enrollees about the doula benefit and workforce issues. MACPAC, “Doulas in Medicaid: Case Study Findings,” November 2023, https://www.macpac.gov/wp-content/uploads/2023/11/Doulas-in-Medicaid-Case-Study-Findings.pdf. To help address these concerns, the N.J. Department of Health convened the New Jersey Doula Learning Collaborative in 2022, which, through the support of HealthConnect One, is providing training, workforce development, supervision support, mentoring, technical assistance, direct billing, and sustainability planning for community doulas and doula organizations throughout the state. Also in 2022, CMS approved N.J.’s amended State Medicaid Plan to increase the reimbursement rate for maternity service clinicians and community doulas. National Health Law Program, “Current State Doula Medicaid Efforts,” https://healthlaw.org/doulamedicaidproject/.
[64] New Jersey Department of Human Services, Division of Medical Assistance & Health Services, “Medicaid/NJ FamilyCare Coverage of Doula Services Revised Billing Codes,” February 2021, https://www.nj.gov/humanservices/dmahs/info/Newsletter_31-04_Doula.pdf.
[65] Oregon SPA #17-0006, CMS Approval letter and Approved SPA. David L. Meacham, Letter to Lynne Saxton, Department of Health and Human Services, Division of Medicaid and Children’s Health Operations, July 19, 2017, https://www.medicaid.gov/sites/default/files/State-resource-center/Medicaid-State-Plan-Amendments/Downloads/OR/OR-17-0006.pdf.
[66] Carl Rush, Elinor Higgins, and Sandra Wilkniss, “State Approaches to Community Health Worker Financing through Medicaid State Plan Amendments,” National Academy for State Health Policy, December 7, 2022, https://nashp.org/state-approaches-to-community-health-worker-financing-through-medicaid-state-plan-amendments/.
[67] Ibid.
[68] Social Security Act § 2105(a)(1)(D)(ii). State spending on HSIs counts toward the overall 10 percent cap on spending for administrative expenses, which also includes the cost of administering the program, outreach, and other activities. As of July 2019, 24 states had one or more approved HSIs. See Medicaid and CHIP Payment and Access Commission, “CHIP Health Services Initiatives: What They Are and How States Use Them,” July 2019, https://www.macpac.gov/wp-content/uploads/2019/07/CHIP-Health-Services-Initiatives.pdf. For a description of services and supports considered allowable under CHIP HSIs, see CMS, “Coverage of Health-Related Social Needs Services in Medicaid and the Children’s Health Insurance Program,” November 2023, https://www.medicaid.gov/sites/default/files/2023-11/hrsn-coverage-table.pdf.
[69] Anita Cardwell, “Leveraging CHIP to Improve Children’s Health: An Overview of State Health Services Initiatives,” National Academy for State Health Policy, May 20, 2019, https://nashp.org/leveraging-chip-to-improve-childrens-health-an-overview-of-state-health-services-initiatives/.
[70] Federal Match Rates for Medicaid Administrative Activities, 42 CFR 432.50; 42 CFR 435.15. See Medicaid and CHIP Payment and Access Commission, “Federal Match Rates for Medicaid Administrative Activities,” https://www.macpac.gov/federal-match-rates-for-medicaid-administrative-activities/. Most administrative expenditures are matched at 50 percent, but certain activities are eligible for a higher matching rate, such as investments in translation services (matched at 75 percent) and health information technology (matched at 90 percent).
[71] Costello, op. cit.
[72] Veronnica Thompson and Anoosha Hasan, “Medicaid Reimbursement for Home Visiting Services,” National Academy for State Health Policy, May 1, 2023, https://nashp.org/medicaid-reimbursement-for-home-visiting-services/.
[73] Michigan leaders also used contract incentives to expand access to community-based providers. Medicaid MCO plans in Michigan are required to contract with at least one community health worker for every 5,000 members. See Michigan Department of Health and Human Services, “State of Michigan Contract No. Comprehensive Health Care Program for the Michigan Department of Health and Human Services,” 2021, https://www.michigan.gov/mdhhs/-/media/Project/Websites/mdhhs/Folder1/Folder101/contract_7696_7.pdf .
[74] State of Illinois, “Model Contract,” January 24, 2018, https://interactives.commonwealthfund.org/medicaidmcdb/contracts/IL1_201824001MCOModelContractRev3RedLine.pdf?_gl=1*tqf6dn*_gcl_au*MTU0ODUxNzU5OC4xNjg3NTM4MjM4.
[75] Florida Medicaid Managed Care Contract; see the Agency of Health Care Administration, “Attachment II Exhibit II-A – Update: February 1, 2022 Managed Medical Assistance (MMA) Program,” p. 40, https://ahca.myflorida.com/content/download/9938/file/Exhibit_II_A_MMA-2022-02-01.pdf.
[76] MassHealtb, Accountable Care Partnership Plan Contracts, https://www.mass.gov/lists/accountable-care-partnership-plan-contracts.
[77] Oregon Health Authority, “Health-Related Services Guide for CCOs: Traditional Health Workers and Health-Related Services,” updated November 2022, https://www.oregon.gov/oha/HPA/dsi-tc/Documents/Health-Related-Services-Guide-THWs.pdf.
[78] Oregon Health Authority, “Oregon Medicaid Fee-for-Service reimbursement for Community Health Workers,” updated September 1, 2020, https://www.oregon.gov/oha/HSD/OHP/Tools/CHW_Billing%20Guide.pdf.
[79] Oregon Health Authority, 2022, op. cit.
[80] Ibid.
[81] Tricia Brooks, “Measuring and Improving Health Care Quality for Children in Medicaid and CHIP: A Primer for Child Health Stakeholders,” Georgetown University Health Policy Institute Center for Children and Families, March 2016, https://ccf.georgetown.edu/wp-content/uploads/2016/03/Measuring_Health_Quality_Medicaid_CHIP_Primer.pdf.
[82] Ibid.
[83] Medicaid.gov, “2023 Core Set of Adult Health Care Quality Measures for Medicaid (Adult Core Set),” https://www.medicaid.gov/sites/default/files/2023-08/2023-adult-core-set_0.pdf.
[84] Medicaid.gov, “2023 Core Set of Children’s Health Care Quality Measures for Medicaid and CHIP (Child Core Set),” https://www.medicaid.gov/sites/default/files/2023-08/2023-child-core-set_0.pdf.
[85] Medicaid.gov, “2023 Core Set of Maternal and Perinatal Health Measures for Medicaid and CHIP (Maternity Core Set),” https://www.medicaid.gov/sites/default/files/2023-08/2023-maternity-core-set.pdf.
[86] Kathryn R. Fingar et al., “Reassessing the Association between WIC and Birth Outcomes Using a Fetuses-at-Risk Approach,” Maternal Child Health Journal, Vol. 21, No. 4, April 2017, https://pubmed.ncbi.nlm.nih.gov/27531011/. For a discussion of additional research on the relationship between WIC participation and birthweight, see Steven Carlson and Zoë Neuberger, “WIC Works: Addressing the Nutrition and Health Needs of Low-Income Families for More Than Four Decades,” CBPP, updated January 27, 2021, https://www.cbpp.org/sites/default/files/atoms/files/5-4-15fa.pdf.
[87] Recent USDA-sponsored research following mothers and children who enrolled in WIC as infants shows that nearly all (95 percent) have a doctor’s office, health clinic, or other medical facility that they visit for routine physical examinations and wellness checks by the time their child nears his or her 4th birthday. Tracy Thomas et al., “Assessing Immunization Interventions in the Women, Infants, and Children (WIC) Program,” American Journal of Preventive Medicine, Vol. 47, No. 5, November 2014, https://doi.org/10.1016/j.amepre.2014.06.017.
[88] Tim Bersak and Lyudmyla Sonchak, “The impact of WIC on infant immunizations and healthcare utilization,” Health Services Research, Vol. 53, S1, August 2018, https://doi.org/10.1111/1475-6773.12810; Thomas et al., op. cit.
[89] Federal Register “Medicaid Program and CHIP; Mandatory Medicaid and Children's Health Insurance Program (CHIP) Core Set Reporting,” August 31, 2023, https://www.federalregister.gov/documents/2023/08/31/2023-18669/medicaid-program-and-chip-mandatory-medicaid-and-childrens-health-insurance-program-chip-core-set.
[90] EPSDT also requires coverage of medically necessary “interperiodic” screening outside of the state’s periodicity schedule. Coverage for such screenings is required based on an indication of a medical need to diagnose an illness or condition that was not present at the regularly scheduled screening or to determine if there has been a change in a previously diagnosed illness or condition that requires additional services. The determination of whether an interperiodic screen is medically necessary may be made by a health, developmental, or educational professional who comes into contact with the child outside of the formal health care system (e.g., state early intervention or special education programs, Head Start and day care programs, WIC, and other nutritional assistance programs). This includes, for example, personnel working for state early intervention or special education programs, Head Start, and WIC. A state may not limit the number of medically necessary screenings a child receives and may not require prior authorization for either periodic or interperiodic screenings. See Department of Health and Human Services, “EPSDT - A Guide for States: Coverage in the Medicaid Benefit for Children and Adolescents,” June 2014, https://www.medicaid.gov/sites/default/files/2019-12/epsdt_coverage_guide.pdf.
[91] There are different ways that states can provide rewards or payments to plans that are beyond the scope of this paper. Shilpa Patel and Laurie C. Zephyrin, “Medicaid Managed Care Opportunities to Promote Health Equity in Primary Care,” Commonwealth Fund, December 19, 2022, https://www.commonwealthfund.org/blog/2022/medicaid-managed-care-opportunities-promote-health-equity-primary-care.
[92] Oregon Health Authority, “CCO Incentive Metrics & WIC,” https://www.oregon.gov/oha/PH/HEALTHYPEOPLEFAMILIES/WIC/Documents/cco-metrics-wic.pdf.
[93] Oregon’s Coordinated Care Organizations are built on the foundation of Oregon’s MCOs, but have multiple features that distinguish them from MCOs: CCOs are locally governed, with representation from Medicaid members, health care providers, and other local stakeholders.
[94] Oregon Health Authority, “2023 CCO Quality Incentive Program: Measure Summaries,” January 2023, https://www.oregon.gov/oha/HPA/ANALYTICS/CCOMetrics/PlainLanguageIncentiveMeasures.pdf.
[95] Oregon Health Authority, “SDOH Screening & Referral Metric: Frequently Asked Questions,” updated September 2023, https://www.oregon.gov/oha/HPA/dsi-tc/Documents/SDOH-Screening-Metric-FAQ.pdf.
[96] State of Pennsylvania, Department of Human Services, “2023 Community HealthChoices Agreement,” January 2023, https://www.dhs.pa.gov/HealthChoices/HC-Services/Documents/2023%20HealthChoices%20Agreement%20including%20Exhibits%20and%20Non-financial%20Appendices.pdf.
[97] CMS, “CMS Strategic Plan,” September 27, 2023, https://www.cms.gov/cms-strategic-plan.
[98] Anne Marie Costello, Letter to State Health Officials, January 7, 2021https://www.medicaid.gov/federal-policy-guidance/downloads/sho21001.pdf.
[99] CMS, “Health Related Social Needs,” https://www.medicaid.gov/health-related-social-needs/index.html.
[100] Daniel Tsai, Letter to State Medicaid Directors, Centers for Medicare & Medicaid Services, January 4, 2023. “https://www.medicaid.gov/federal-policy-guidance/downloads/smd23001.pdfIn lieu of” services can be used at the option of the managed care plan and the enrollee as long as they are a cost-effective substitute for state plan services and settings.
[101] Centers for Medicare & Medicaid Services, Medicaid and Children’s Health Insurance Program (CHIP) Managed Care Access, Finance, and Quality Proposed Rule, 88 Fed. Reg. 28092, May 3, 2023, https://www.govinfo.gov/content/pkg/FR-2023-05-03/pdf/2023-08961.pdf.
[102] Office of Disease Prevention and Health Promotion, HHS, “White House Challenge to End Hunger and Build Healthy Communities,” https://health.gov/our-work/nutrition-physical-activity/white-house-conference-hunger-nutrition-and-health/make-commitment#:~:text=Invest%20in%20health%2Drelated%20social,about%20nutrition%20and%20physical%20activity
[103] No Kid Hungry, “Share Our Strength Announces Commitments in Support of the White House Conference on Hunger, Nutrition and Health,” September 28, 2022, www.nokidhungry.org/who-we-are/pressroom/share-our-strength-announces-commitments-support-white-house-conference-hunger#:~:text=By%202030%2C%20the%20American%20Academy,federal%20and%20community%20nutrition%20resources.
[104] No Kid Hungry, “No Kid Hungry providing 14 state AAP chapters with $280,000 in grants to fuel strategy,” December 13, 2022, https://www.nokidhungry.org/who-we-are/pressroom/release-no-kid-hungry-and-american-academy-pediatrics-expand-partnership.
[105] American Academy of Pediatrics, “WIC Program,” Pediatrics, Vol. 108, Issue 5, November 1, 2001, https://publications.aap.org/pediatrics/article-abstract/108/5/1216/63773/WIC-Program?redirectedFrom=fulltext.
[106] Ibid.
[107] The American College of Obstetricians and Gynecologists, “Importance of Social Determinants of Health and Cultural Awareness in the Delivery of Reproductive Health Care,” Committee Opinion, Number 729, January 2018, https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2018/01/importance-of-social-determinants-of-health-and-cultural-awareness-in-the-delivery-of-reproductive-health-care.
[108] CommunityRX could be programmed to include referrals to local WIC programs. Stacy Tessler Lindau et al., “Building and experimenting with an agent-based model to study the population-level impact of CommunityRx, a clinic-based community resource referral intervention,” PLOS Computational Biology, Vol. 17, No. 10, 2021, https://doi.org/10.1371/journal.pcbi.1009471.
[109] The clinic served 14,000 patients with more than 90 percent enrolled in Medicaid. Bryan Monroe et al., “Assessing and Improving WIC Enrollment in the Primary Care Setting: A Quality Initiative,” Pediatrics, Vol. 152, No. 2, August 2023, https://publications.aap.org/pediatrics/article/152/2/e2022057613/192532/Assessing-and-Improving-WIC-Enrollment-in-the?autologincheck=redirected.
[110] Brittany Goldstein et al., “Integration of Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) in Primary Care Settings,” Journal of Community Health, September 2023, https://link.springer.com/article/10.1007/s10900-023-01287-5.
[111] Erin R. Hager et al., “Development and validity of a 2-item screen to identify families at risk for food insecurity,” Pediatrics, Vol.126, No. 1, July 2010, https://doi.org/10.1542/peds.2009-3146.
[112] Although an affirmative response to both questions increases the likelihood of food insecurity existing in the household, an affirmative response to only one question is often an indication of food insecurity and should prompt additional questioning. See Benjamin Gitterman et al., “Promoting Food Security for All Children,” Pediatrics, Vol 136, Issue 5, November 2015, https://publications.aap.org/pediatrics/article/136/5/e1431/33896/Promoting-Food-Security-for-All-Children?autologincheck=redirected. USDA also has an 18-question measure to assess food insecurity with the Household Food Security Scale, which is the standard tool for research, but may not be necessary for making referrals to programs like WIC for food assistance. Alisha Coleman-Jensen et al., “Household Food Security in the United States in 2013,” USDA, Economic Research Service, September 2014, https://www.ers.usda.gov/publications/pub-details/?pubid=102075.
[113] For more information about tracking and coding systems, see Sheila Smith et al., “Medicaid Policies to Help Young Children Access Key Infant-Early Childhood Mental Health Services: Results From A 50-State Survey,” National Center for Children in Poverty at Bank Street Graduate School of Education, Georgetown University McCourt School of Public Policy, Center for Children and Families, and Johnson Policy Consulting, June 2022, p. 3, https://www.nccp.org/wp-content/uploads/2023/06/NCCP-Medicaid-Brief_6.13.23-FINAL.pdf.
[114] Petry S. Urbi et al., “The Role of State Policy in Use of Z Codes to Document Social Need in Medicaid Data,” NORC, March 2022, https://www.norc.org/PDFs/Documentation%20of%20Social%20Needs%20in%202018%20Medicaid%20Data/The%20Role%20of%20State%20Medicaid%20Policy%20in%20Documentation%20of%20SDOH%20in%20Medicaid%20Data_032422.pdf.
[115] Bailit Health, “Addressing Health-Related Social Needs Through Medicaid Managed Care,” Health Foundation of South Florida, October 2022, https://www.shvs.org/wp-content/uploads/2022/11/Addressing-HRSN-Through-Medicaid-Managed-Care_October-2022.pdf.
[116] North Carolina Department of Health and Human Services, “Screening Questions.”
[117] North Carolina Department of Health and Human Services, “Healthy Opportunities.”
[118] Medicaid and CHIP Payment and Access Commission, “Quality requirements under Medicaid managed care,” https://www.macpac.gov/subtopic/quality-requirements-under-medicaid-managed-care/.
[119] For more information about PIPs that focus on improvements in pregnancy, see Andy Schneider et al., “Medicaid Managed Care, Maternal Mortality Review Committees, and Maternal Health: A 12-State Scan,” Georgetown University McCourt School of Public Policy, Center for Children and Families, October 2023, https://ccf.georgetown.edu/2023/10/16/medicaid-managed-care-maternal-mortality-review-committees-and-maternal-health-a-12-state-scan/.
[120] Division of TennCare, “2021 Update To The Quality Assessment And Performance Improvement Strategy,” https://www.tn.gov/content/dam/tn/tenncare/documents/qualitystrategy.pdf.
[121] Minnesota Department of Human Services, “Contract for Prepaid Medical Assistance and Minnesota Care,” January 1, 2022, https://mn.gov/dhs/assets/2022-fc-model-contract_tcm1053-515037.pdf, For more information, see Stratis Health, “Performance Improvement Project (PIP): Healthy Start for Minnesota Children,” https://stratishealth.org/health-plan-performance-improvement-projects-pips/pip-healthy-start-for-minnesota-children/.
[122] Maggie Clark, “State Trends to Leverage Medicaid Extended Postpartum Coverage, Benefits and Payment Policies to Improve Maternal Health,” Georgetown University McCourt School of Public Policy, Center for Children and Families, March 20, 2023, https://ccf.georgetown.edu/2023/03/20/state-trends-to-leverage-medicaid-extended-postpartum-coverage-benefits-and-payment-policies-to-improve-maternal-health/.
More from the Authors

Areas of Expertise

Areas of Expertise
