BEYOND THE NUMBERS
The “Supercommittee” and Medicare
As the new congressional deficit-reduction committee considers proposals to cut Medicare spending, it needs to keep two critical — but often overlooked — facts in mind.
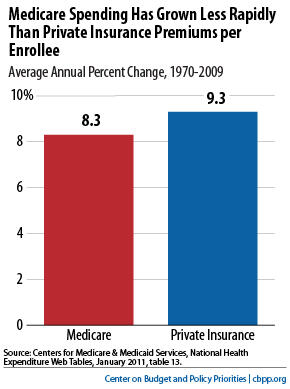
First, the problem of rising health costs affects the entire health care system, public and private. In recent decades, Medicare and private-sector health care costs have grown at about the same rate per beneficiary (see chart), which shouldn’t be surprising since they use the same doctors, hospitals, and medical procedures. In fact, Medicare has been a leader in adopting cost-control policies that private insurers have then widely adopted.
To achieve these savings, the ACA establishes a host of new initiatives that aim to transform Medicare into a program that rewards health care providers based on the value of their care, not the volume of their procedures. These include bundling payments for episodes of care, reducing avoidable hospital readmissions, testing and implementing new ways to increase the value of care, coordinating care under Medicare and Medicaid, informing patients and payers about the quality of health care providers, and increasing funding for comparative effectiveness research. The law also creates an Independent Payment Advisory Board that will develop and submit proposals to reduce cost growth and improve quality in both Medicare and the health care system as a whole.
These reforms will take time to plan, test, and implement. But they can succeed only if we give them a chance, and that won’t happen if health reform opponents succeed in repealing them.
Even if all of the ACA’s savings materialize, we’ll need to do more over the long run to slow the growth of health care costs in the private and public sectors alike. In the near term, however, achieving large additional savings will be difficult, since the ACA includes most of the good ideas for slowing the growth of Medicare spending. Other proposals, like increasing the age of eligibility for Medicare or replacing the program with vouchers that wouldn’t keep pace with health costs, would generally just shift costs to beneficiaries, states, and employers — and in many cases would increase total health care spending.
Given the limited possibilities for more Medicare cuts in the next five to ten years, the congressional “supercommittee” needs to develop a balanced package of deficit-reduction measures, including significant additional revenues, to reach its goal of achieving $1.2 to $1.5 trillion in deficit savings over the next ten years.
