BEYOND THE NUMBERS
Medicaid and State Budgets
As we’ve noted, the new Ravitch-Volcker report outlines some of the long-term structural budget problems that states face. The report’s discussion of Medicaid raises some important points but could also leave readers with a mistaken impression about Medicaid’s role in state budgets.
The report agrees with other independent analyses that the Affordable Care Act’s (ACA) Medicaid expansion is a good deal for states:
For states that want to increase coverage for the uninsured, ACA is a bargain. The federal government will pay 100 percent of the cost of covering the newly eligible enrollees beginning in 2014, phasing down to 90 percent in 2019. Since ACA’s enactment, there has been significant research on the estimated annual cost to states of its implementation. The Kaiser Commission on Medicaid and the Uninsured has projected average additional state spending over the pre-ACA baseline of 1.4 percent by 2019, while a study by the Lewin Group estimate increased state spending of 1.1 percent. (Report of the State Budget Crisis Task Force, p. 20)
It also recommends that federal and state governments work together to control rising health care costs as well as Medicaid costs. We very much agree.
Rising health care costs affect both public programs like Medicaid and Medicare as well as private insurance, since both publicly and privately funded health care are delivered largely by the same providers in the same settings and use the same procedures and medications.
Moreover, Medicaid spending per beneficiary has grown more slowly than private insurance premiums over the last decade. Medicaid coverage also costs considerably less per beneficiary than private coverage because of Medicaid’s lower payment rates to providers and lower administrative costs.
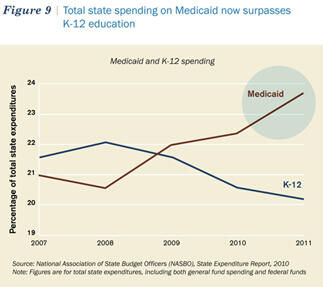
Unfortunately, the Ravitch-Volcker report doesn’t make clear that state Medicaid spending — while growing — is still a distant second behind state spending on K-12 education. The graph below, which we’ve reproduced from the report, seems to show the opposite, but its measure of “total state spending” includes spending financed by both federal Medicaid funds and state revenues.
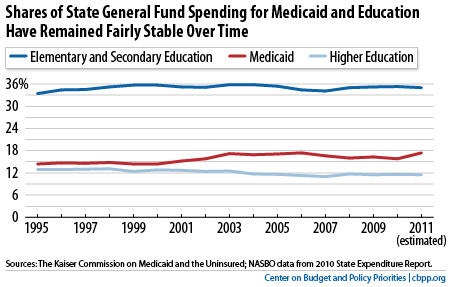
Looking just at state general funds — where states place most of their own revenues — is a more appropriate measure of Medicaid’s role in state budgets and paints a different picture. Measured as a share of state general funds, state Medicaid spending was less than half of state spending on K-12 education in 2011, as the graph below shows. The graph also shows that Medicaid and K-12 spending have remained relatively steady over time as a share of state general fund budgets.
Slowing the growth in Medicaid costs is a critical mid- and long-term issue for state budgets, but it requires a system-wide approach. Fortunately, the ACA takes a number of steps to test new approaches for delivering care in Medicare and Medicaid that hold the promise of lowering cost growth while improving quality. If they prove successful, they can and should be adopted more widely throughout the U.S. health care system, including in state Medicaid programs.
