BEYOND THE NUMBERS
Another Misguided Charge Against Health Reform
Critics claim that the new health reform law’s expansion of Medicaid eligibility will place heavy new financial burdens on states and prompt large numbers of insured people to drop their private coverage for Medicaid. The first claim is incorrect, as I explained recently, and here’s why the second one is too:
In recent years, a dozen states have expanded Medicaid to cover adults with incomes at or above the poverty line. If expanding Medicaid really “crowd outs” private insurance to a large degree, these states should have significantly lower rates of private coverage among low-income adults than other states.
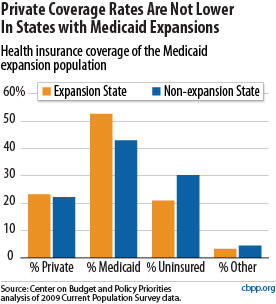
Moreover, the expansion states have a much lower proportion of low-income residents who are uninsured (21 percent compared to 30 percent).
In other words, expanding Medicaid has reduced the ranks of the uninsured without undermining private coverage.
Similarly, several research studies have found little or no crowd-out when states expand public health insurance programs.
One likely reason is that many low- and moderate-income people don’t have access to private health coverage in the first place. In 2005, just 34 percent of non-elderly workers with incomes below the poverty line were offered coverage through their job. And many of those offered coverage can’t take it because they can’t afford the premiums.
What all this means is that the vast majority of the 16 million adults and children that the Congressional Budget Office estimates will gain Medicaid coverage by 2019 under the health reform expansion would have otherwise been uninsured.
